Platta Christopher S, Wallace Charlie, Gondi Vinai, Das Rupak, Straub Margaret, Al-Niaimi Ahmed, Applegate Glenn, Bradley Kristin A
Department of Human Oncology, University of Wisconsin Hospital and Clinics, Madison, USA.
Department of Human Oncology, University of Wisconsin Hospital and Clinics, Madison, USA ; CDH Cancer Center, Madison, USA.
J Contemp Brachytherapy. 2014 Mar;6(1):76-81. doi: 10.5114/jcb.2014.40768. Epub 2014 Feb 19.
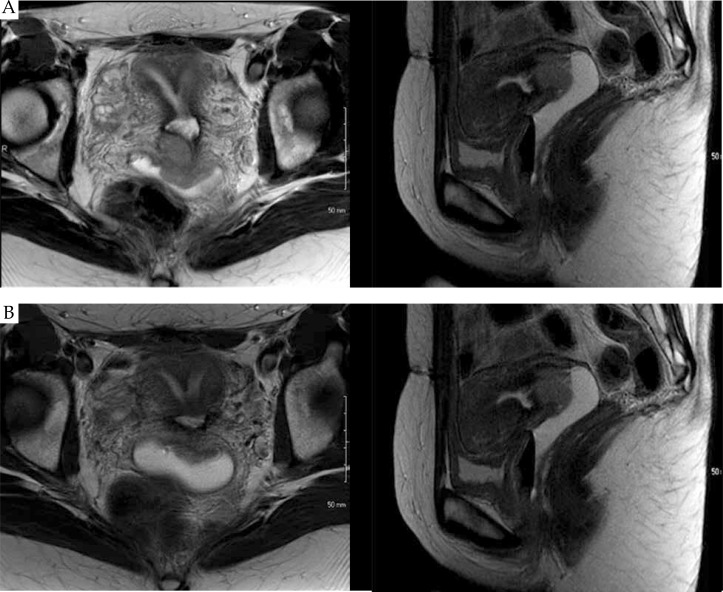
To describe an approach to cervical brachytherapy in a patient with congenital septate uterus and locally advanced cervical carcinoma.
The patient is a 34-year-old female with septate uterus presenting with pelvic pain. Workup demonstrated a stage IIB cervical adenocarcinoma with imaging evidence of an involved right external iliac lymph node. The patient received whole pelvic radiation, with concurrent weekly cisplatin (40 mg/m(2)), to a dose of 45 Gy in 25 fractions followed by a parametrial boost of 5.4 Gy and an additional nodal boost of 9 Gy.
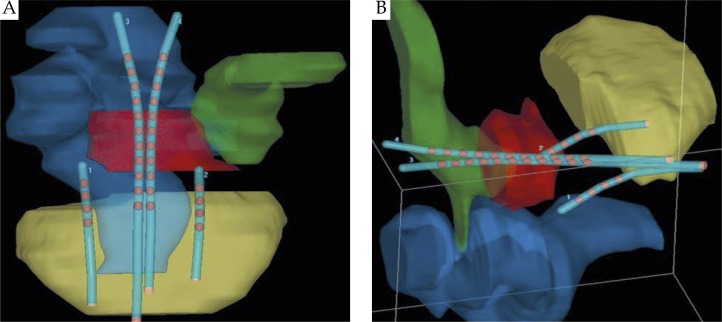
The patient was initiated on cervical brachytherapy following fraction 23 of pelvic radiation. To conform to her septated uterus, a Rotte-Y tandem was used. Additionally, 2 CT-compatible ovoids were placed in the vaginal apex to enhance dose distribution and coverage of the target volume. Each fraction of brachytherapy was performed with CT-based planning. A high-risk clinical target volume (HR-CTV) and normal structures were defined and constrained per American Brachytherapy Society (ABS) and Groupe Européen de Curiethérapie/European Society for Therapeutic Radiology and Oncology (GEC-ESTRO) guidelines. The brachytherapy dose was 27.5 Gy in 5 fractions of 5.5 Gy each, prescribed to the HR-CTV.
Herein, we report the first documented case of cervical brachytherapy in a patient with septate uterus and locally advanced cervical carcinoma. Using CT-guided planning, in conjunction with the ABS and GEC-ESTRO guidelines, the patient was effectively treated with adapted cervical brachytherapy, meeting criteria for HR-CTV coverage and normal tissue tolerances.
描述对一名患有先天性纵隔子宫和局部晚期宫颈癌患者进行宫颈近距离放射治疗的方法。
该患者为一名34岁患有纵隔子宫的女性,伴有盆腔疼痛。检查显示为IIB期宫颈腺癌,影像学证据表明右侧髂外淋巴结受累。患者接受了全盆腔放疗,同时每周给予顺铂(40mg/m²),剂量为45Gy,分25次照射,随后对宫旁组织追加5.4Gy照射,对淋巴结额外追加9Gy照射。
患者在盆腔放疗第23次后开始进行宫颈近距离放射治疗。为适应她的纵隔子宫,使用了Rotte-Y形施源器。此外,在阴道顶端放置了2个与CT兼容的卵形容器,以增强剂量分布和靶区覆盖。每次近距离放射治疗均采用基于CT的计划。根据美国近距离放射治疗学会(ABS)和欧洲放射治疗与肿瘤学会(GEC-ESTRO)的指南定义并限制了高危临床靶区(HR-CTV)和正常组织。近距离放射治疗剂量为27.5Gy,分5次,每次5.5Gy,处方剂量给予HR-CTV。
在此,我们报告了首例有记录的对患有纵隔子宫和局部晚期宫颈癌患者进行宫颈近距离放射治疗的病例。通过使用CT引导的计划,并结合ABS和GEC-ESTRO指南,该患者通过适应性宫颈近距离放射治疗得到了有效治疗,达到了HR-CTV覆盖标准和正常组织耐受标准。