Lai J C, Feng S, Terrault N A, Lizaola B, Hayssen H, Covinsky K
Division of Gastroenterology and Hepatology, Department of Medicine, University of California-San Francisco, San Francisco, CA.
Am J Transplant. 2014 Aug;14(8):1870-9. doi: 10.1111/ajt.12762. Epub 2014 Jun 16.
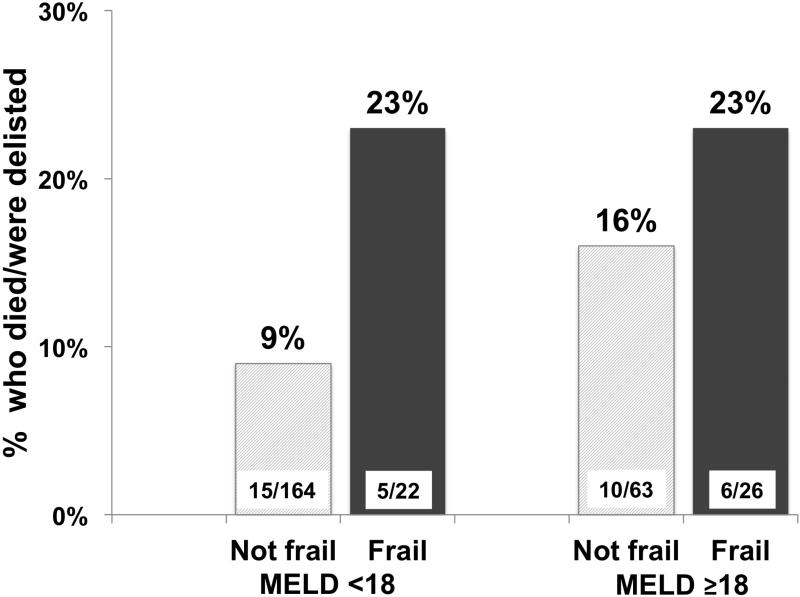
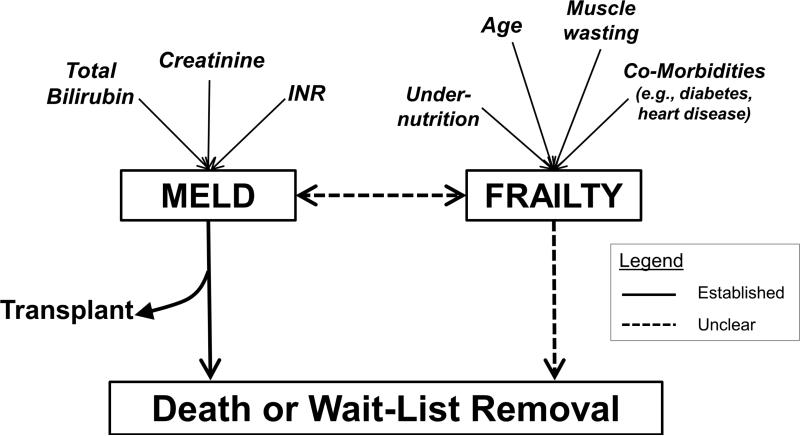
We aimed to determine whether frailty, a validated geriatric construct of increased vulnerability to physiologic stressors, predicts mortality in liver transplant candidates. Consecutive adult outpatients listed for liver transplant with laboratory Model for End-Stage Liver Disease (MELD) ≥ 12 at a single center (97% recruitment rate) underwent four frailty assessments: Fried Frailty, Short Physical Performance Battery (SPPB), Activities of Daily Living (ADL) and Instrumental ADL (IADL) scales. Competing risks models associated frailty with waitlist mortality (death/delisting for being too sick for liver transplant). Two hundred ninety-four listed liver transplant patients with MELD ≥ 12, median age 60 years and MELD 15 were followed for 12 months. By Fried Frailty score ≥3, 17% were frail; 11/51 (22%) of the frail versus 25/243 (10%) of the not frail died/were delisted (p = 0.03). Each 1-unit increase in the Fried Frailty score was associated with a 45% (95% confidence interval, 4-202) increased risk of waitlist mortality adjusted for MELD. Similarly, the adjusted risk of waitlist mortality associated with each 1-unit decrease (i.e. increasing frailty) in the Short Physical Performance Battery (hazard ratio 1.19, 95% confidence interval 1.07-1.32). Frailty is prevalent in liver transplant candidates. It strongly predicts waitlist mortality, even after adjustment for liver disease severity demonstrating the applicability and importance of the frailty construct in this population.
我们旨在确定衰弱这一已得到验证的、表明对生理应激源易感性增加的老年医学概念,是否能预测肝移植候选者的死亡率。在一个中心,连续的成年门诊肝移植候选者(终末期肝病模型(MELD)实验室指标≥12,招募率97%)接受了四项衰弱评估:Fried衰弱评估、简短体能状况量表(SPPB)、日常生活活动(ADL)量表和工具性日常生活活动(IADL)量表。竞争风险模型将衰弱与等待名单上的死亡率(因病情过重无法进行肝移植而死亡/被除名)相关联。对294例MELD≥12、中位年龄60岁且MELD评分为15的登记肝移植患者进行了为期12个月的随访。根据Fried衰弱评分≥3,17%的患者为衰弱患者;衰弱患者中有11/51(22%)死亡/被除名,而非衰弱患者中有25/243(10%)死亡/被除名(p = 0.03)。Fried衰弱评分每增加1个单位,经MELD调整后的等待名单死亡率风险增加45%(95%置信区间,4 - 202)。同样,简短体能状况量表每降低1个单位(即衰弱程度增加),经调整后的等待名单死亡率风险增加(风险比1.19,95%置信区间1.07 - 1.32)。衰弱在肝移植候选者中普遍存在。即使在对肝病严重程度进行调整后,它仍能强烈预测等待名单上的死亡率,这表明衰弱概念在该人群中的适用性和重要性。