Moore Kenneth T, Vaidyanathan Seema, Natarajan Jaya, Ariyawansa Jay, Haskell Lloyd, Turner Kenneth C
Janssen Research and Development, LLC, Titusville, NJ, USA.
J Clin Pharmacol. 2014 Dec;54(12):1407-20. doi: 10.1002/jcph.352. Epub 2014 Jul 3.
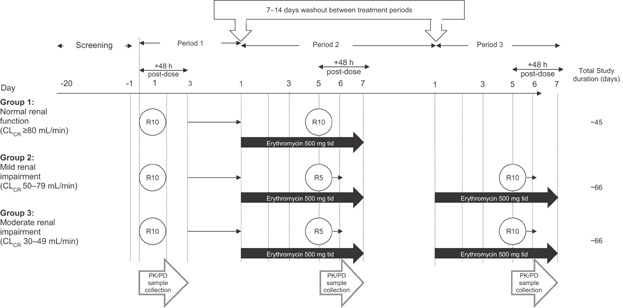
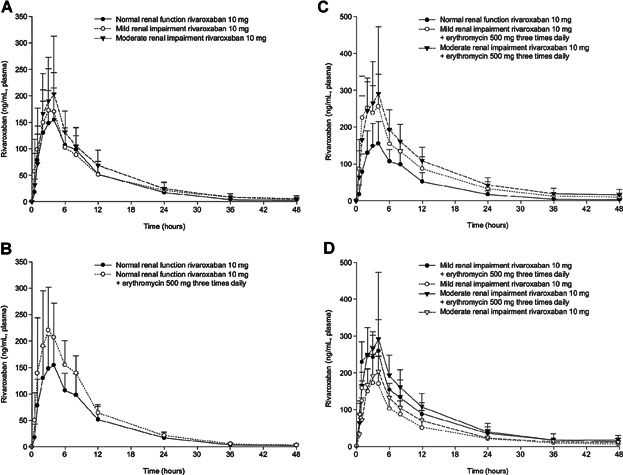
Two previously conducted rivaroxaban studies showed that, separately, renal impairment (RI) and concomitant administration of erythromycin (P-glycoprotein and moderate cytochrome P450 3A4 [CYP3A4] inhibitor) can result in increases in rivaroxaban exposure. However, these studies did not assess the potential for combined drug-drug-disease interactions, which-in theory-could lead to additive or synergistic increases in exposure. This study investigated rivaroxaban pharmacokinetics and pharmacodynamics when co-administered with steady-state (SS) erythromycin in subjects with either mild or moderate RI. Similar to previous studies, rivaroxaban administered alone in RI subjects, or when co-administered with SS erythromycin in normal renal function (NRF) subjects, increased rivaroxaban exposure. When combined, the co-administration of rivaroxaban 10 mg with SS erythromycin in subjects with mild or moderate RI produced mean increases in rivaroxaban AUC∞ and Cmax of approximately 76% and 56%, and 99% and 64%, respectively, relative to NRF subjects, with PD changes displaying a similar trend. No serious adverse events occurred and no persistent adverse events were reported at the end of study. Although these increases were slightly more than additive, rivaroxaban should not be used in patients with RI receiving concomitant combined P-glycoprotein and moderate CYP3A4 inhibitors, unless the potential benefit justifies the potential risk.
之前进行的两项利伐沙班研究分别表明,肾功能损害(RI)以及与红霉素(一种P-糖蛋白和中度细胞色素P450 3A4[CYP3A4]抑制剂)同时给药可导致利伐沙班暴露量增加。然而,这些研究并未评估联合药物-药物-疾病相互作用的可能性,理论上这种相互作用可能导致暴露量的累加或协同增加。本研究调查了在轻度或中度RI患者中,利伐沙班与稳态(SS)红霉素合用时的药代动力学和药效学。与之前的研究相似,单独给予RI患者利伐沙班,或在肾功能正常(NRF)的患者中与SS红霉素合用时,利伐沙班的暴露量均增加。联合使用时,在轻度或中度RI患者中,10mg利伐沙班与SS红霉素合用后,相对于NRF患者,利伐沙班的AUC∞和Cmax平均分别增加约76%和56%,以及99%和64%,药效学变化呈现相似趋势。研究结束时未发生严重不良事件,也未报告持续性不良事件。尽管这些增加幅度略大于累加效应,但除非潜在获益证明潜在风险合理,否则RI患者接受P-糖蛋白和中度CYP3A4抑制剂联合给药时不应使用利伐沙班。