De Knijf A, Pattinson R C
Registrar, Department of Obstetrics and Gynaecology, KULeuven, Belgium.
MRC Maternal and Infant Health Care Strategies Research Unit, Department of Obstetrics and Gynaecology, University of Pretoria, Kalafong Hospital, Pretoria, South Africa.
Facts Views Vis Obgyn. 2010;2(4):219-25.
To identify avoidable factors contributing to neonatal morbidity and mortality due to "birth asphyxia" and to ascertain if hypoxic ischemic encephalopathy (HIE) alone could act as a good marker for avoidable factors associated with "birth asphyxia".
Kalafong Hospital, South Africa, a regional hospital unit that caters for mainly indigent urban population but also receives referrals from the Mpumalanga Province.
All neonates and intrapartum stillbirths fulfilling the criteria of birth asphyxia born at the Kalafong Hospital during 2008 and 2009 were included. Neonates born at less than 34 weeks gestation, born with infection, major congenital malformations or inborn errors of metabolism and intrapartum deaths due to abruption placentae were excluded. Neonates referred from Level 1 clinics postnatally, who qualified with these criteria, were also included in the study. The files were retrieved, and avoidable factors were identified. Avoidable factors were classified into 3 groups: patient associated, administrative and medical personnel associated problems.
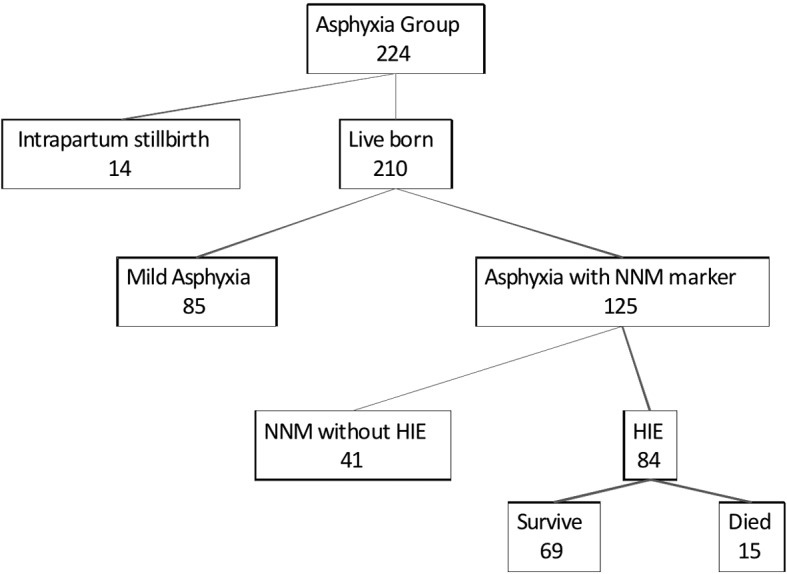
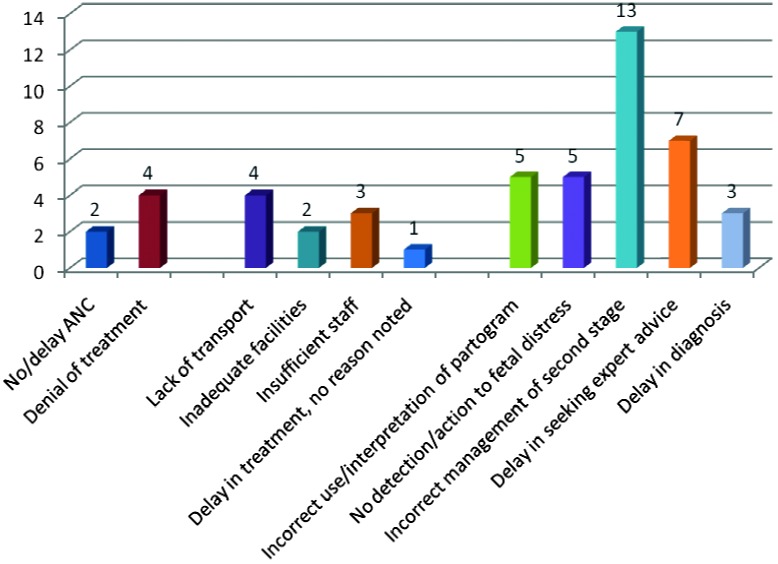
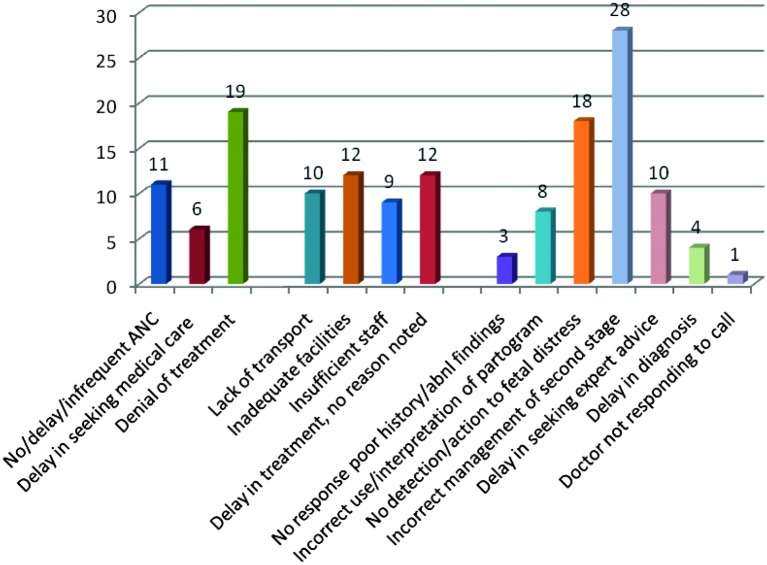
In 2008 and 2009, 10117 babies were born at Kalafong Hospital. 224 babies with intrapartum related asphyxia were identified (22.1/1000 births). This group consisted of 14 intrapartum stillbirths, 85 neonates with mild asphyxia, 125 babies with severe asphyxia of which 41 had a neonatal near miss markers without HIE and 84 with HIE. Fifteen of the babies with HIE subsequently died. The number of avoidable factors identified per case file reviewed increased with the severity of the hypoxic event, mild asphyxia 0.74, neonatal near miss without HIE 0.85, HIE survivor 0.91, and stillbirth or neonatal death 1.29. Major avoidable factors for birth asphyxia were refusal of medical treatment, inadequate facilities, no detection of or reaction to fetal distress, and incorrect management of second stage. The avoidable factors detected in neonates with HIE were the same as those detected in the whole group.
The avoidable factors described in a confidential enquiry concentrating on the labour management of women delivering neonates with all grades of "birth asphyxia" were similar to those found in women delivering neonates with HIE. HIE in neonates is a clearly defined condition, making it a good marker to use to review the quality of intrapartum care received by the women who delivered neonates with HIE.
确定导致“出生窒息”所致新生儿发病和死亡的可避免因素,并确定单纯的缺氧缺血性脑病(HIE)是否可作为与“出生窒息”相关的可避免因素的良好指标。
南非卡拉方医院,这是一家地区医院,主要服务贫困城市人口,也接收来自姆普马兰加省的转诊患者。
纳入2008年和2009年在卡拉方医院出生且符合出生窒息标准的所有新生儿和产时死产儿。排除孕周小于34周、伴有感染、严重先天性畸形或先天性代谢缺陷出生的新生儿以及因胎盘早剥导致的产时死亡。产后从一级诊所转诊且符合这些标准的新生儿也纳入研究。检索病历,确定可避免因素。可避免因素分为3组:患者相关、行政和医务人员相关问题。
2008年和2009年,卡拉方医院共出生10117名婴儿。确定224例产时相关窒息婴儿(22.1/1000例出生)。该组包括14例产时死产儿、85例轻度窒息新生儿、125例重度窒息婴儿,其中41例有新生儿濒死标志物但无HIE,84例有HIE。15例有HIE的婴儿随后死亡。每例审查病历中确定的可避免因素数量随缺氧事件严重程度增加,轻度窒息为0.74,无HIE的新生儿濒死为0.85,HIE存活者为0.91,死产或新生儿死亡为1.29。出生窒息的主要可避免因素为拒绝治疗、设施不足、未检测到或未对胎儿窘迫做出反应以及第二产程管理不当。HIE新生儿中检测到的可避免因素与整个组中检测到的相同。
在一项针对分娩各级“出生窒息”新生儿的产程管理的保密调查中描述的可避免因素,与分娩HIE新生儿的产妇中发现的因素相似。新生儿HIE是一种明确界定的病症,使其成为用于审查分娩HIE新生儿的产妇所接受的产时护理质量的良好指标。