Gonzalez-Casanova Ines, Sarmiento Olga Lucia, Pratt Michael, Gazmararian Julie A, Martorell Reynaldo, Cunningham Solveig A, Stein Aryeh
Hubert Department of Global Health, Rollins School of Public Health, Nutrition and Health Sciences Program, Emory University, 1518 Clifton Rd NE, 7000H, Atlanta, GA 30322. E-mail:
Facultad de Medicina, Universidad de los Andes, Bogotá, Colombia.
Prev Chronic Dis. 2014 Aug 7;11:E134. doi: 10.5888/pcd11.140065.
Information from high-income countries is often used to design childhood obesity prevention interventions in low- and middle-income countries, even though determinants may differ greatly between settings.
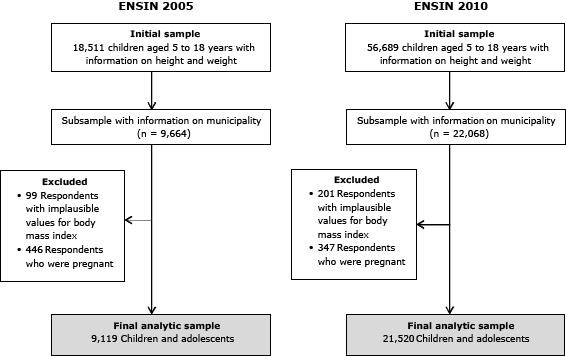
We examined the associations of individual, family (household), and community (municipality) characteristics with body mass index (BMI) z scores and likelihood of overweight among children aged 5 to 18 years measured for the Colombian National Nutrition surveys of 2005 (n = 9,119) and 2010 (n = 21,520). We used 3-level hierarchical linear models with child as level 1, household as level 2, and municipality as level 3.
The prevalence of combined overweight and obesity among Colombian children and adolescents was 15.7% in 2005 and 16.6% in 2010. The household level explained 40% in 2005 and 31% in 2010 of the variability in BMI z scores. Wealth was positively associated with BMI in 2005 (0.09 increase in z score per wealth quintile) and 2010 (0.13 increase in z score per wealth quintile) (P < .01). Children and adolescents from extended families had higher BMI z scores than those from nuclear families; BMI z scores were inversely associated with the number of family members living in the same household. The municipality level explained only between 2% and 3% of the variability in BMI. Income inequality was positively associated with BMI z scores in 2010.
These patterns differ from those commonly described in high-income countries and suggest more appropriate opportunities for interventions to prevent child and adolescent obesity in Colombia and other Latin American settings and populations.
尽管不同环境下儿童肥胖的决定因素可能差异很大,但来自高收入国家的信息常被用于设计低收入和中等收入国家的儿童肥胖预防干预措施。
我们研究了2005年(n = 9119)和2010年(n = 21520)哥伦比亚全国营养调查中测量的5至18岁儿童个体、家庭(住户)和社区(市)特征与体重指数(BMI)z评分及超重可能性之间的关联。我们使用了三级分层线性模型,其中儿童为第一层,家庭为第二层,市为第三层。
2005年哥伦比亚儿童和青少年超重与肥胖合并患病率为15.7%,2010年为16.6%。家庭层面在2005年解释了BMI z评分变异性的40%,在2010年解释了31%。2005年(每财富五分位数z评分增加0.09)和2010年(每财富五分位数z评分增加0.13),财富与BMI呈正相关(P <.01)。来自大家庭的儿童和青少年的BMI z评分高于核心家庭的儿童和青少年;BMI z评分与同一家庭居住的家庭成员数量呈负相关。市层面仅解释了BMI变异性的2%至3%。2010年,收入不平等与BMI z评分呈正相关。
这些模式与高收入国家通常描述的模式不同,表明在哥伦比亚和其他拉丁美洲环境及人群中,有更合适的机会进行预防儿童和青少年肥胖的干预。