Kandula Namratha R, Kanaya Alka M, Liu Kiang, Lee Ji Young, Herrington David, Hulley Stephen B, Persell Stephen D, Lloyd-Jones Donald M, Huffman Mark D
Northwestern University, Chicago, IL (N.R.K., K.L., J.Y.L., S.D.P., D.M.L.J., M.D.H.).
University of California, San Francisco, CA (A.M.K., S.B.H.).
J Am Heart Assoc. 2014 Oct 2;3(5):e001117. doi: 10.1161/JAHA.114.001117.
Ten-year and lifetime cardiovascular risk assessment algorithms have been adopted into atherosclerotic cardiovascular disease (ASCVD) prevention guidelines, but these prediction models are not based on South Asian populations and may underestimate the risk in Indians, Pakistanis, Bangladeshis, Nepali, and Sri Lankans in the United States. Little is known about ASCVD risk prediction and intermediate endpoints such as subclinical atherosclerosis in US individuals of South Asian ancestry.
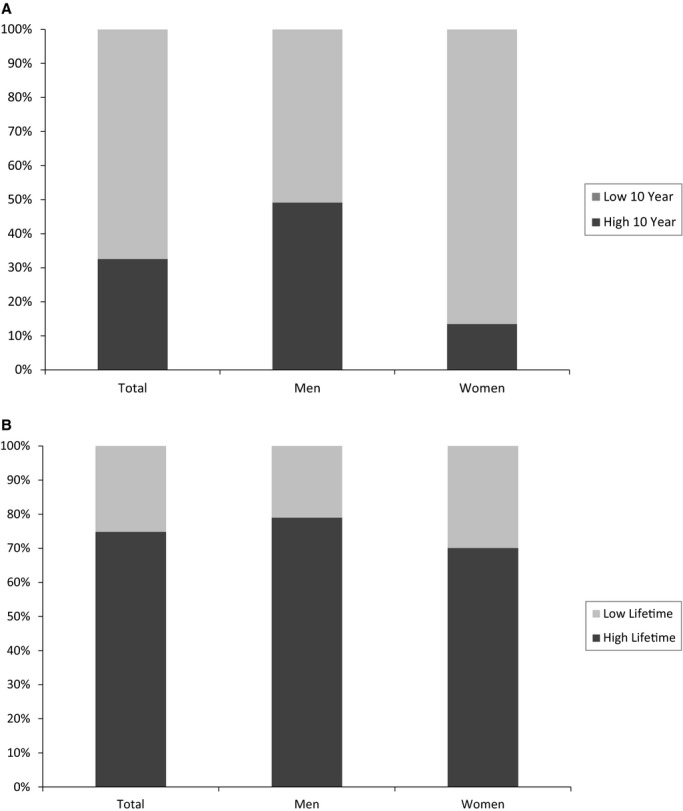
South Asians (n=893) from the Mediators of Atherosclerosis in South Asians Living in America (MASALA) study who were 40 to 79 years and free of ASCVD were included. Ten-year ASCVD predicted risk was calculated using the 2013 Pooled Cohort Equations. Lifetime predicted risk was based on risk factor burden. Baseline levels of subclinical atherosclerosis (coronary artery calcium [CAC] and carotid intima media thickness [CIMT]) were compared across 10-year and lifetime risk strata: (1) high (≥7.5%) 10-year and low (<7.5%) 10-year risk; (2) high (≥39%) lifetime and low (<39%) lifetime risk. South Asian men and women with high 10-year predicted risk had a significantly greater CAC burden than those with low 10-year risk. South Asians with high lifetime predicted risk had a significantly increased odds for CAC higher than 0 (odds ratio: men 1.97; 95% CI, 1.2 to 3.2; women 3.14; 95% CI, 1.5, 6.6). Associations between risk strata and CIMT were also present.
This study is the first to provide evidence that contemporary ASCVD risk assessment algorithms derived from non-Hispanic white and African-American samples can successfully identify substantial differences in atherosclerotic burden in US South Asians.
十年期和终生心血管风险评估算法已被纳入动脉粥样硬化性心血管疾病(ASCVD)预防指南,但这些预测模型并非基于南亚人群,可能会低估在美国的印度人、巴基斯坦人、孟加拉国人、尼泊尔人和斯里兰卡人的风险。对于美国南亚裔个体的ASCVD风险预测以及诸如亚临床动脉粥样硬化等中间终点知之甚少。
纳入了来自美国南亚人动脉粥样硬化介质(MASALA)研究的893名40至79岁且无ASCVD的南亚人。使用2013年合并队列方程计算十年期ASCVD预测风险。终生预测风险基于风险因素负担。在十年期和终生风险分层中比较亚临床动脉粥样硬化(冠状动脉钙化[CAC]和颈动脉内膜中层厚度[CIMT])的基线水平:(1)十年期高风险(≥7.5%)和十年期低风险(<7.5%);(2)终生高风险(≥39%)和终生低风险(<39%)。十年期预测风险高的南亚男性和女性的CAC负担明显高于十年期风险低的人群。终生预测风险高的南亚人CAC高于0的几率显著增加(优势比:男性1.97;95%CI,1.2至3.2;女性3.14;95%CI,1.5,6.6)。风险分层与CIMT之间也存在关联。
本研究首次提供证据表明,源自非西班牙裔白人和非裔美国人样本的当代ASCVD风险评估算法能够成功识别美国南亚人动脉粥样硬化负担的显著差异。