Sood Beena G, Keszler Martin, Garg Meena, Klein Jonathan M, Ohls Robin, Ambalavanan Namasivayam, Cotten C Michael, Malian Monica, Sanchez Pablo J, Lakshminrusimha Satyan, Nelin Leif D, Van Meurs Krisa P, Bara Rebecca, Saha Shampa, Das Abhik, Wallace Dennis, Higgins Rosemary D, Shankaran Seetha
Department of Pediatrics, Children's Hospital of Michigan, 3901 Beaubien Blvd., 4H42, Detroit, MI, 48201, USA.
Department of Pediatrics, Women and Infants Hospital, Brown University, 101 Dudley Street, Providence, RI, 0290, USA.
Trials. 2014 Dec 12;15:486. doi: 10.1186/1745-6215-15-486.
Inhaled nitric oxide (INO), a selective pulmonary vasodilator, has revolutionized the treatment of neonatal hypoxemic respiratory failure (NHRF). However, there is lack of sustained improvement in 30 to 46% of infants. Aerosolized prostaglandins I2 (PGI2) and E1 (PGE1) have been reported to be effective selective pulmonary vasodilators. The objective of this study was to evaluate the feasibility of a randomized controlled trial (RCT) of inhaled PGE1 (IPGE1) in NHRF.
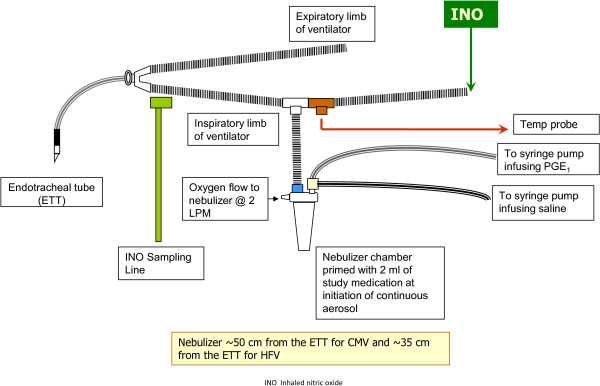
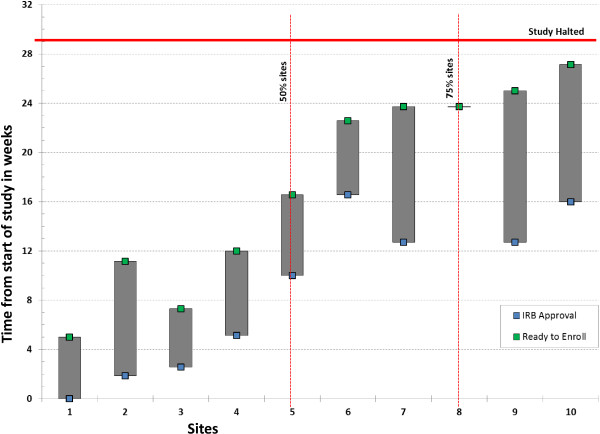
Two pilot multicenter phase II RCTs are included in this report. In the first pilot, late preterm and term neonates with NHRF, who had an oxygenation index (OI) of ≥15 and <25 on two arterial blood gases and had not previously received INO, were randomly assigned to receive two doses of IPGE1 (300 and 150 ng/kg/min) or placebo. The primary outcome was the enrollment of 50 infants in six to nine months at 10 sites. The first pilot was halted after four months for failure to enroll a single infant. The most common cause for non-enrollment was prior initiation of INO. In a re-designed second pilot, co-administration of IPGE1 and INO was permitted. Infants with suboptimal response to INO received either aerosolized saline or IPGE1 at a low (150 ng/kg/min) or high dose (300 ng/kg/min) for a maximum duration of 72 hours. The primary outcome was the recruitment of an adequate number of patients (n = 50) in a nine-month-period, with fewer than 20% protocol violations.
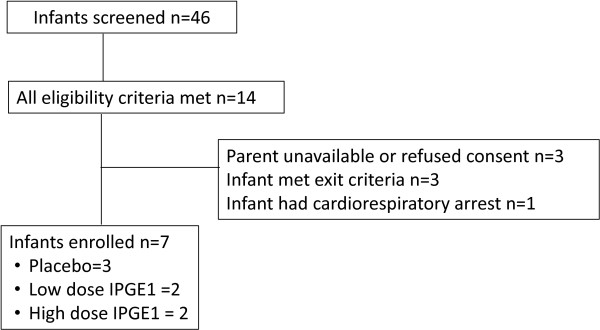
No infants were enrolled in the first pilot. Seven patients were enrolled in the second pilot; three in the control, two in the low-dose IPGE1, and two in the high-dose IPGE1 groups. The study was halted for recruitment futility after approximately six months as enrollment targets were not met. No serious adverse events, one minor protocol deviation and one pharmacy protocol violation were reported.
These two pilot RCTs failed to recruit adequate eligible newborns with NHRF. Complex management RCTs of novel therapies for persistent pulmonary hypertension of the newborn (PPHN) may require novel study designs and a longer period of time from study approval to commencement of enrollment.
CLINICALTRIALS.GOV: Pilot one: NCT number: 00598429 registered on 10 January 2008. Last updated: 3 February 2011. Pilot two: NCT number: 01467076 17 October 2011. Last updated: 13 February 2013.
吸入一氧化氮(INO)作为一种选择性肺血管扩张剂,彻底改变了新生儿低氧性呼吸衰竭(NHRF)的治疗方式。然而,46%的婴儿病情未得到持续改善。雾化前列腺素I2(PGI2)和前列腺素E1(PGE1)据报道是有效的选择性肺血管扩张剂。本研究的目的是评估吸入PGE1(IPGE1)治疗NHRF的随机对照试验(RCT)的可行性。
本报告纳入两项Ⅱ期多中心预试验RCT。在第一项预试验中,患有NHRF的晚期早产儿和足月儿,在两次动脉血气分析中氧合指数(OI)≥15且<25,且此前未接受过INO治疗,被随机分配接受两剂IPGE1(300和150 ng/kg/min)或安慰剂。主要结果是在10个地点6至9个月内招募50名婴儿。第一项预试验在4个月后因未能招募到一名婴儿而停止。未招募的最常见原因是之前已开始使用INO。在重新设计的第二项预试验中,允许联合使用IPGE1和INO。对INO反应欠佳的婴儿接受雾化生理盐水或低剂量(150 ng/kg/min)或高剂量(300 ng/kg/min)的IPGE1,最长持续72小时。主要结果是在9个月内招募足够数量的患者(n = 50),方案违背率低于20%。
第一项预试验未招募到婴儿。第二项预试验招募了7名患者;3名在对照组,2名在低剂量IPGE1组,2名在高剂量IPGE1组。由于未达到招募目标,该研究在大约6个月后因招募无效而停止。未报告严重不良事件,报告了1项轻微方案偏离和1项药房方案违背。
这两项预试验RCT未能招募到足够数量符合条件的NHRF新生儿。针对新生儿持续性肺动脉高压(PPHN)新疗法的复杂管理随机对照试验可能需要新的研究设计以及从研究获批到开始招募的更长时间。
CLINICALTRIALS.GOV:预试验一:NCT编号:00598429,于2008年1月10日注册。最后更新:2011年2月3日。预试验二:NCT编号:01467076,于2011年10月17日注册。最后更新:2013年2月13日。