Ho Cheng-Maw, Hu Rey-Heng, Lee Po-Huang, Wu Yao-Ming, Ho Ming-Chih
From the Department of Surgery (C-MH, R-HH, P-HL, Y-MW, M-CH), National Taiwan University Hospital; and Graduate Institute of Clinical Medicine (C-MH, P-HL), College of Medicine, National Taiwan University, Taipei, Taiwan.
Medicine (Baltimore). 2014 Dec;93(27):e203. doi: 10.1097/MD.0000000000000203.
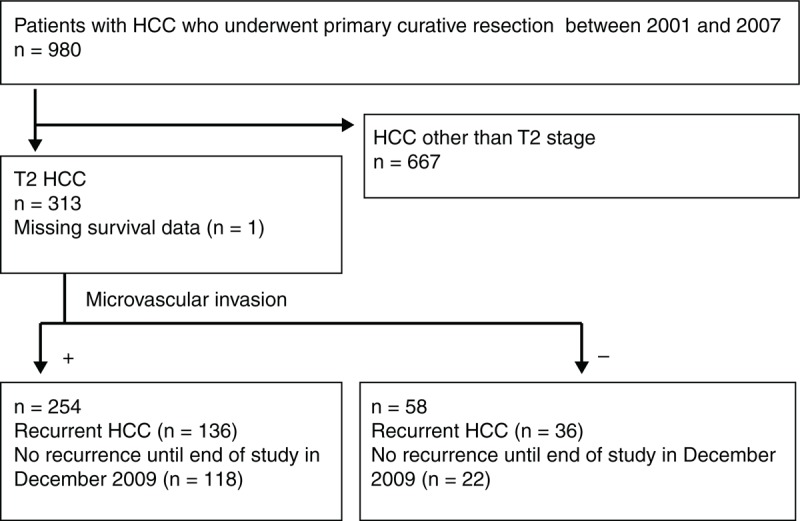
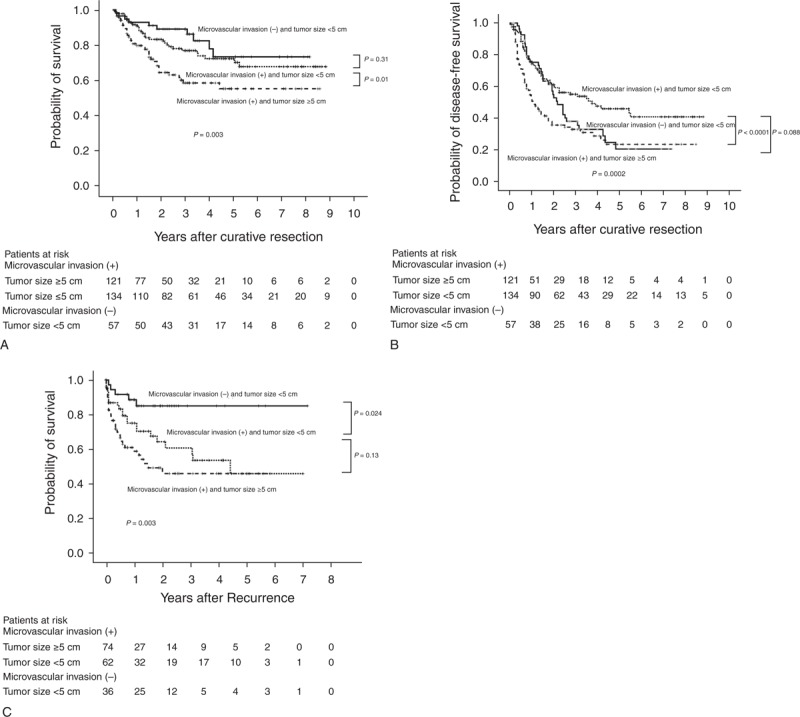
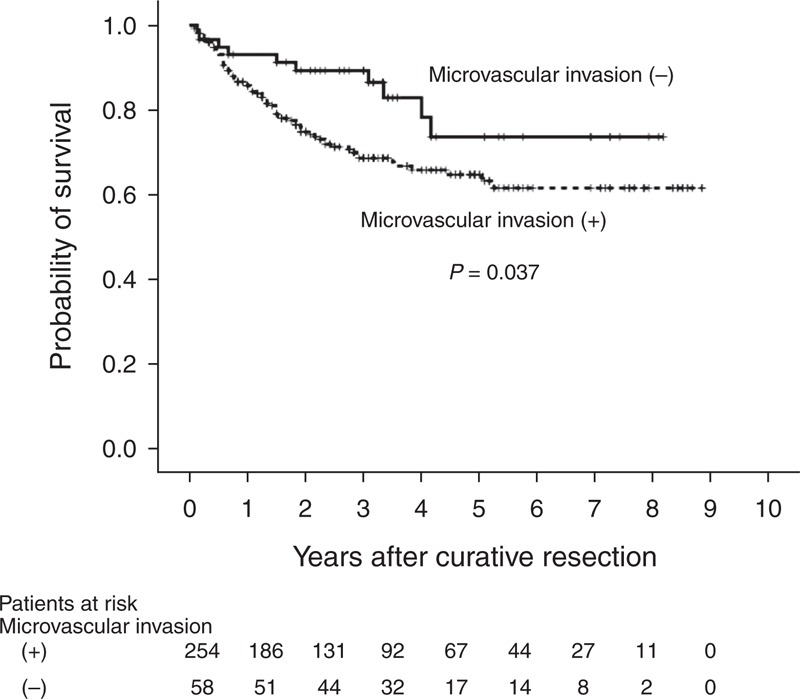
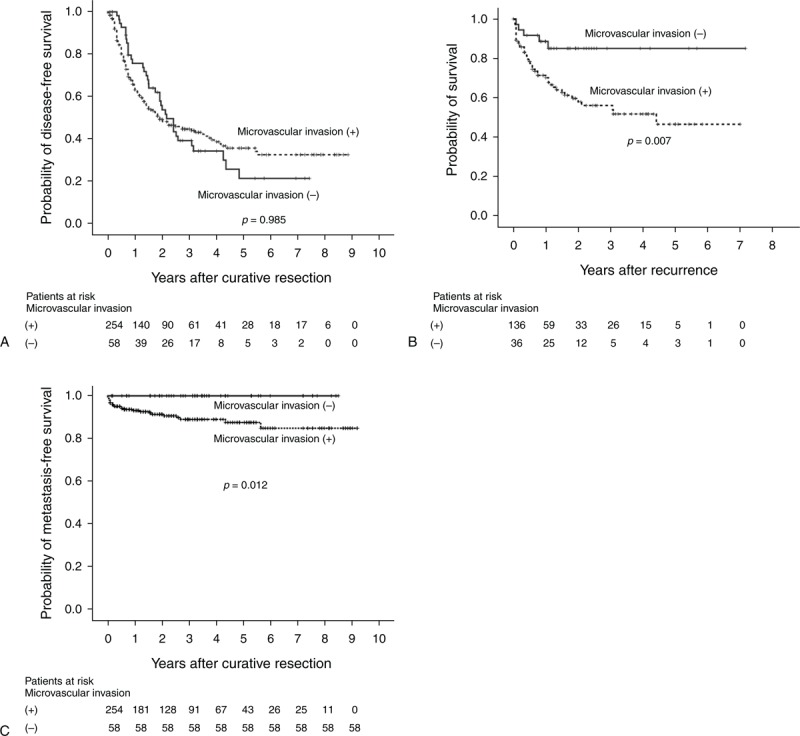
Insufficient data are available regarding the validation of long-term survival in patients with T2 (solitary tumor with microvascular invasion [MVI] or multiple tumors, none >5 cm) hepatocellular carcinoma (HCC) after primary hepatectomy. We aim to evaluate the survival and relevant risk factors for T2 HCC patients. Between 2001 and 2007, 312 T2 HCC patients who underwent primary hepatectomy were included. Survival was estimated using the Kaplan-Meier method and compared using Cox proportional hazard model with adjusted independent prognostic factors. The 1, 3, and 5-year overall survival rates of patients with MVI were 85.7%, 68.7%, and 64.8%, respectively; these were inferior to the rates in patients without MVI, which were 93.0%, 89.3%, and 73.7%, respectively (P = 0.037). Within the with-MVI group, the survival rate of patients with tumor sizes ≥ 5 cm was inferior to that of patients with tumors <5 cm (overall, P = 0.01; recurrence-free, P < 0.0001). For patients with the largest tumors in the <5-cm group, those without MVI tended to have a higher probability of recurrence for 2 years after resection (P = 0.088) but a similar overall survival rate relative to those with MVI (P = 0.31). The crude metastasis-free survival was higher in the without-MVI group than in the with-MVI group (P = 0.012). The T2 HCC category comprised heterogeneous patients with differences in survival rates. Extrahepatic recurrence occurred more frequently in patients with MVI than in those without MVI. These results provide evidence for an updated definition of T2 HCC.
关于T2期(孤立性肿瘤伴微血管侵犯[MVI]或多发肿瘤,最大径均≤5 cm)肝细胞癌(HCC)患者肝切除术后长期生存情况的验证,目前可用数据不足。我们旨在评估T2期HCC患者的生存情况及相关危险因素。2001年至2007年期间,纳入了312例行肝切除术的T2期HCC患者。采用Kaplan-Meier法估计生存率,并使用Cox比例风险模型比较,对独立预后因素进行校正。MVI患者的1年、3年和5年总生存率分别为85.7%、68.7%和64.8%;低于无MVI患者的相应生存率,分别为93.0%、89.3%和73.7%(P = 0.037)。在MVI组中,肿瘤大小≥5 cm患者的生存率低于肿瘤<5 cm患者(总体,P = 0.01;无复发生存率,P < 0.0001)。对于肿瘤最大径<5 cm组的患者,无MVI者在切除术后2年复发概率较高(P = 0.088),但总生存率与有MVI者相似(P = 0.31)。无MVI组的无远处转移生存率高于MVI组(P = .012)。T2期HCC患者存在异质性,生存率有所不同。MVI患者肝外复发比无MVI患者更常见。这些结果为T2期HCC的更新定义提供了依据。