Straub Rainer H
Arthritis Res Ther. 2014 Nov 13;16 Suppl 2(Suppl 2):S4. doi: 10.1186/ar4688.
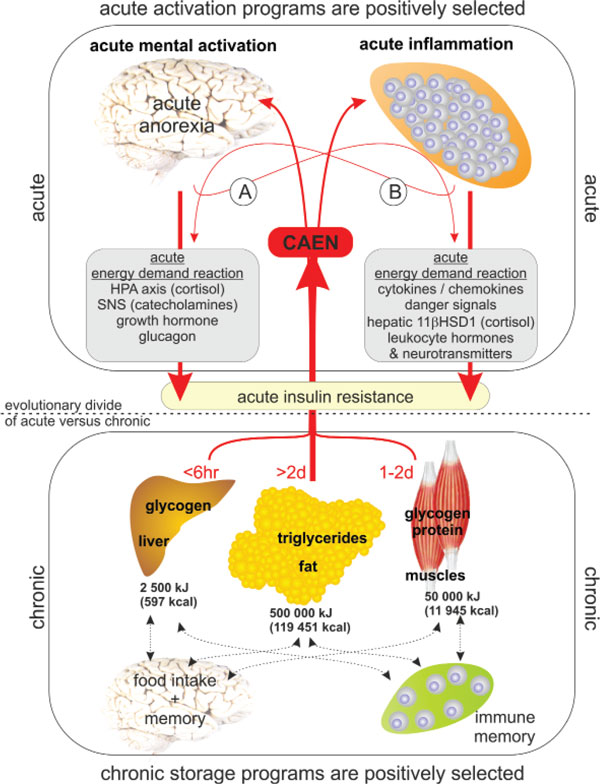
Insulin resistance (IR) is a general phenomenon of many physiological states, disease states, and diseases. IR has been described in diabetes mellitus, obesity, infection, sepsis, trauma, painful states such as postoperative pain and migraine, schizophrenia, major depression, chronic mental stress, and others. In arthritis, abnormalities of glucose homeostasis were described in 1920; and in 1950 combined glucose and insulin tests unmistakably demonstrated IR. The phenomenon is now described in rheumatoid arthritis, systemic lupus erythematosus, ankylosing spondylitis, polymyalgia rheumatica, and others. In chronic inflammatory diseases, cytokine-neutralizing strategies normalize insulin sensitivity. This paper delineates that IR is either based on inflammatory factors (activation of the immune/ repair system) or on the brain (mental activation via stress axes). Due to the selfishness of the immune system and the selfishness of the brain, both can induce IR independent of each other. Consequently, the immune system can block the brain (for example, by sickness behavior) and the brain can block the immune system (for example, stress-induced immune system alterations). Based on considerations of evolutionary medicine, it is discussed that obesity per se is not a disease. Obesity-related IR depends on provoking factors from either the immune system or the brain. Chronic inflammation and/or stress axis activation are thus needed for obesity-related IR. Due to redundant pathways in stimulating IR, a simple one factor-neutralizing strategy might help in chronic inflammatory diseases (inflammation is the key), but not in obesity-related IR. The new considerations towards IR are interrelated to the published theories of IR (thrifty genotype, thrifty phenotype, and others).
胰岛素抵抗(IR)是许多生理状态、疾病状态和疾病中的普遍现象。胰岛素抵抗已在糖尿病、肥胖症、感染、脓毒症、创伤、疼痛状态(如术后疼痛和偏头痛)、精神分裂症、重度抑郁症、慢性精神压力等情况中被描述。在关节炎方面,1920年就描述了葡萄糖稳态异常;1950年,联合葡萄糖和胰岛素测试明确证实了胰岛素抵抗。现在,类风湿性关节炎、系统性红斑狼疮、强直性脊柱炎、风湿性多肌痛等疾病中也描述了这一现象。在慢性炎症性疾病中,细胞因子中和策略可使胰岛素敏感性恢复正常。本文阐述了胰岛素抵抗要么基于炎症因子(免疫/修复系统的激活),要么基于大脑(通过应激轴的精神激活)。由于免疫系统的自主性和大脑的自主性,两者均可独立诱导胰岛素抵抗。因此,免疫系统可阻断大脑(例如,通过疾病行为),大脑也可阻断免疫系统(例如,应激诱导的免疫系统改变)。基于进化医学的考虑,本文讨论了肥胖本身并非一种疾病。与肥胖相关的胰岛素抵抗取决于来自免疫系统或大脑的激发因素。因此,与肥胖相关的胰岛素抵抗需要慢性炎症和/或应激轴激活。由于刺激胰岛素抵抗存在冗余途径,单一的因子中和策略可能对慢性炎症性疾病有帮助(炎症是关键),但对与肥胖相关的胰岛素抵抗无效。对胰岛素抵抗的新思考与已发表的胰岛素抵抗理论(节俭基因型、节俭表型等)相互关联。