Illawarra Health and Medical Research Institute, University of Wollongong, Wollongong, Australia; Graduate School of Medicine, University of Wollongong, Wollongong, Australia.
Karolinska Institute, Department of Cardiothoracic Surgery and Anesthesiology, Karolinska University Hospital, Stockholm, Sweden.
PLoS One. 2015 Apr 2;10(4):e0122838. doi: 10.1371/journal.pone.0122838. eCollection 2015.
Maintenance of high tissue oxygenation (PtO2) is recommended during surgery because PtO2 is highly predictive of surgical site infection and colonic anastomotic leakage. However, surgical site perfusion is often sub-optimal, creating an obstructive hurdle for traditional, systemically applied therapies to maintain or increase surgical site PtO2. This research tested the hypothesis that insufflation of humidified-warm CO2 into the abdominal cavity would increase sub-peritoneal PtO2 during open abdominal surgery.
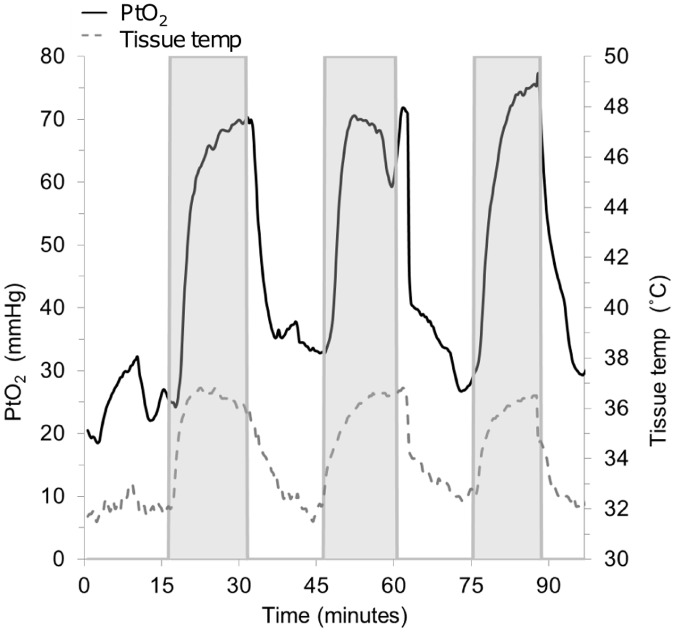
15 Wistar rats underwent laparotomy under general anesthesia. Three sets of randomized cross-over experiments were conducted in which the abdominal cavity was subjected to alternating exposure to 1) humidified-warm CO2 & ambient air; 2) humidified-warm CO2 & dry-cold CO2; and 3) dry-cold CO2 & ambient air. Sub-peritoneal PtO2 and tissue temperature were measured with a polarographic oxygen probe.
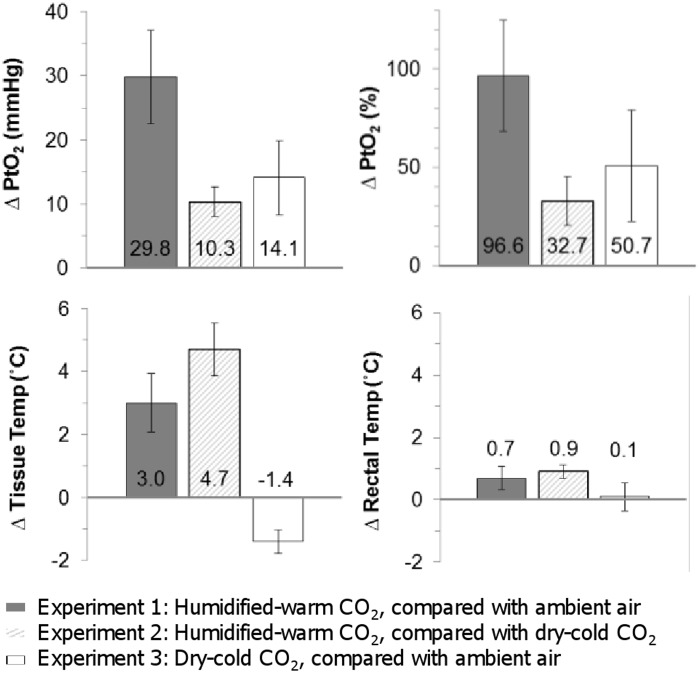
Upon insufflation of humidified-warm CO2, PtO2 increased by 29.8 mmHg (SD 13.3; p<0.001), or 96.6% (SD 51.9), and tissue temperature by 3.0°C (SD 1.7 p<0.001), in comparison with exposure to ambient air. Smaller, but significant, increases in PtO2 were seen in experiments 2 and 3. Tissue temperature decreased upon exposure to dry-cold CO2 compared with ambient air (-1.4°C, SD 0.5, p = 0.001).
In a rat model, insufflation of humidified-warm CO2 into the abdominal cavity during open abdominal surgery causes an immediate and potentially clinically significant increase in PtO2. The effect is an additive result of the delivery of CO2 and avoidance of evaporative cooling via the delivery of the CO2 gas humidified at body temperature.
术中维持组织高氧合(PtO2)被推荐,因为 PtO2 对手术部位感染和结直肠吻合口漏具有高度预测性。然而,手术部位的灌注通常并不理想,这为传统的全身应用治疗方法维持或增加手术部位 PtO2 带来了阻塞性障碍。本研究测试了这样一个假设,即将加湿温热的 CO2 注入腹腔会增加开腹手术时腹膜下的 PtO2。
15 只 Wistar 大鼠在全身麻醉下接受剖腹手术。进行了三组随机交叉实验,其中腹腔依次暴露于 1)加湿温热的 CO2 和环境空气;2)加湿温热的 CO2 和干燥寒冷的 CO2;3)干燥寒冷的 CO2 和环境空气。使用极谱氧探头测量腹膜下 PtO2 和组织温度。
与暴露于环境空气相比,加湿温热的 CO2 注入时 PtO2 增加了 29.8mmHg(SD 13.3;p<0.001),或 96.6%(SD 51.9),组织温度增加了 3.0°C(SD 1.7,p<0.001)。在实验 2 和 3 中,PtO2 也有较小但显著的增加。与暴露于环境空气相比,干燥寒冷的 CO2 暴露时组织温度降低(-1.4°C,SD 0.5,p = 0.001)。
在大鼠模型中,开腹手术时将加湿温热的 CO2 注入腹腔会立即导致 PtO2 显著增加。这种效果是 CO2 输送和避免通过输送加湿至体温的 CO2 气体进行蒸发冷却的附加结果。