Perkins Bruce A, Cherney David Z I, Soleymanlou Nima, Lee Justin A, Partridge Helen, Tschirhart Holly, Zinman Bernard, Mazze Roger, Fagan Nora, Kaspers Stefan, Woerle Hans-Juergen, Broedl Uli C, Johansen Odd Erik
Department of Medicine, Division of Endocrinology and Metabolism, University of Toronto, Toronto, ON, Canada.
Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, Toronto, ON, Canada.
PLoS One. 2015 Nov 6;10(11):e0141085. doi: 10.1371/journal.pone.0141085. eCollection 2015.
We recently reported improved glycemic control with reduced insulin dose in subjects with type 1 diabetes treated with the sodium glucose co-transporter-2 inhibitor empagliflozin. To further characterize the effects, we analyzed diurnal glycemic patterns by continuous glucose monitoring (CGM).
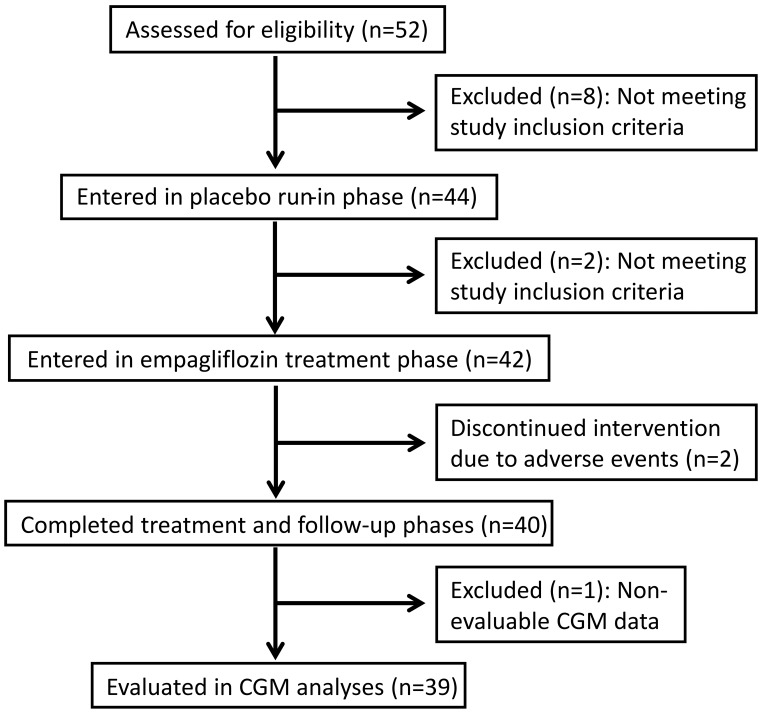
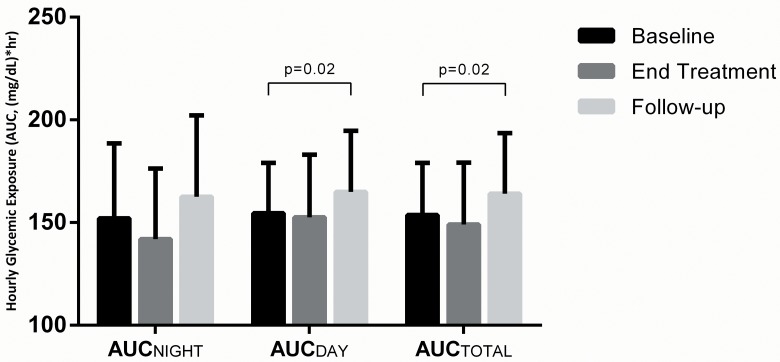
In an 8-week single-arm open-label pilot study of empagliflozin, we compared ambulatory glucose profiles produced from CGM data during 2-week intervals in a placebo run-in baseline period, end-of-treatment, and post-treatment. Change in glycemic exposure was evaluated by area under the median curve according to time of day (AUCTOTAL 12:00am-11:55pm; AUCDAY 7:05am-10:55pm, AUCNIGHT 11:00pm-7:00am), as well as glycemic variability, glycemic stability and time-in-target (≥70 to ≤140mg/dL).
The 40 patients (26 on insulin pump) were aged 24±5 years and BMI 24.5±3.2 kg/m2. Consistent with the observed HbA1c decrease (8.0±0.9% to 7.6±0.9%, p<0.0001), normalized AUCTOTAL CGM decreased from 153.7±25.4 to 149.0±30.2mg/dL∙h at end-of-treatment (p = 0.31), and significantly increased post-treatment (164.1±29.5mg/dL∙h, p = 0.02). The numerical decrease in normalized AUCNIGHT (152.0±36.6 to 141.9±34.4mg/dL∙h, p = 0.13) exceeded AUCDAY (154.5±24.5 to 152.6±30.4mg/dL∙h, p = 0.65). Trends toward lower glycemic variability (83.1±18.9 to 75.6±28.6mg/dL, p = 0.06) and little change in glycemic stability (10.8±3.6 to 10.3±4.5mg/dL/h, p = 0.51) were observed. When empagliflozin was discontinued, these worsened relative to baseline (89.3±19.3mg/dL, p = 0.04 and 11.8±3.7mg/dL/hr, p = 0.08). Time-in-target numerically increased (40.2±11.9 to 43.1±13.5%, p = 0.69) at end-of-treatment but reversed post-treatment. Findings were similar on stratification of pump and MDI subjects.
We observed that empagliflozin was associated with patterns of improved nighttime glycemia more prominent than daytime.
Clinicaltrials.gov NCT01392560.
我们最近报告称,在使用钠-葡萄糖协同转运蛋白2抑制剂恩格列净治疗的1型糖尿病患者中,血糖控制得到改善,胰岛素剂量减少。为了进一步描述其效果,我们通过持续葡萄糖监测(CGM)分析了昼夜血糖模式。
在一项为期8周的恩格列净单臂开放标签试验性研究中,我们比较了在安慰剂导入基线期、治疗结束时和治疗后,每2周间隔期间CGM数据产生的动态血糖谱。根据一天中的时间,通过中位数曲线下面积评估血糖暴露的变化(AUCTOTAL上午12:00至晚上11:55;AUCDAY上午7:05至晚上10:55,AUCNIGHT晚上11:00至上午7:00),以及血糖变异性、血糖稳定性和达标时间(≥70至≤140mg/dL)。
40例患者(26例使用胰岛素泵),年龄24±5岁,体重指数24.5±3.2kg/m²。与观察到的糖化血红蛋白降低情况一致(从8.0±0.9%降至7.6±0.9%,p<0.0001),治疗结束时,标准化的CGM AUCTOTAL从153.7±25.4降至149.0±30.2mg/dL∙h(p = 0.31),治疗后显著增加(164.1±29.5mg/dL∙h,p = 0.02)。标准化的AUCNIGHT数值下降(从152.0±36.6降至141.9±34.4mg/dL∙h,p = 0.13)超过了AUCDAY(从154.5±24.5降至152.6±30.4mg/dL∙h,p = 0.65)。观察到血糖变异性有降低趋势(从83.1±18.9降至75.6±28.6mg/dL,p = 0.06),血糖稳定性变化不大(从10.8±3.6降至10.3±4.5mg/dL/h,p = 0.51)。当停用恩格列净时,这些指标相对于基线恶化(分别为89.3±19.3mg/dL,p = 0.04和11.8±3.7mg/dL/hr,p = 0.08)。治疗结束时达标时间数值增加(从40.2±11.9增至43.1±13.5%,p = 0.69),但治疗后逆转。在胰岛素泵和多次皮下注射胰岛素(MDI)治疗的患者分层分析中,结果相似。
我们观察到,恩格列净与夜间血糖改善模式相关,且这种改善比白天更为显著。
Clinicaltrials.gov NCT01392560。