Lee Yvonne C, Hackett James, Frits Michelle, Iannaccone Christine K, Shadick Nancy A, Weinblatt Michael E, Segurado Oscar G, Sasso Eric H
Division of Rheumatology, Immunology and Allergy, Brigham and Women's Hospital, Boston, MA,
Hackett & Associates Inc., San Diego, CA and.
Rheumatology (Oxford). 2016 Apr;55(4):640-8. doi: 10.1093/rheumatology/kev388. Epub 2015 Nov 25.
To examine the association between a multibiomarker disease activity (MBDA) score, CRP and clinical disease activity measures among RA patients with and without concomitant FM.
In an observational cohort of patients with established RA, we performed a cross-sectional analysis comparing MBDA scores with CRP by rank correlation and cross-classification. MBDA scores, CRP and clinical measures of disease activity were compared between patients with RA alone and RA with concomitant FM (RA and FM) by univariate and multivariate analyses.
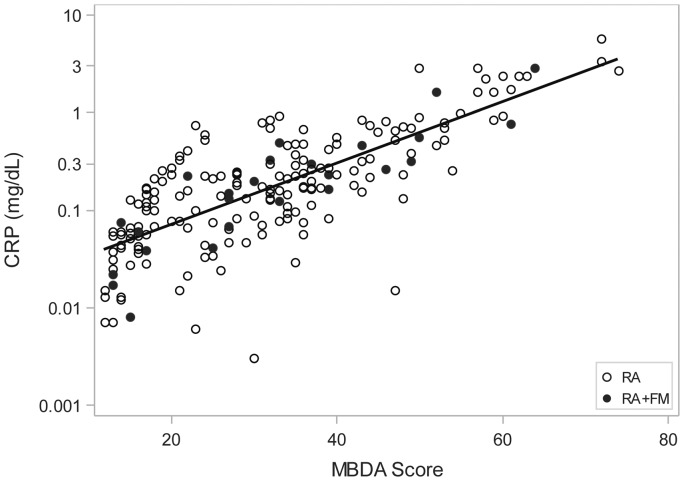
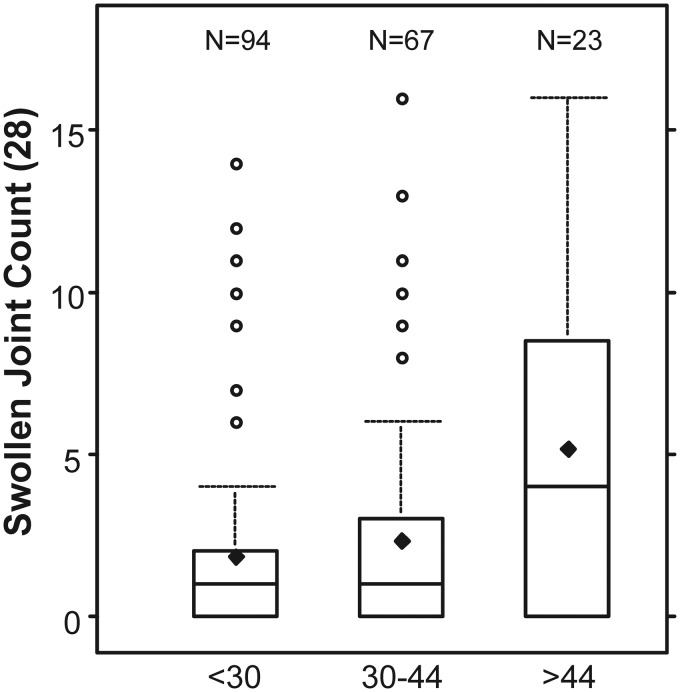
CRP was ⩽1.0 mg/dl for 184 of 198 patients (93%). MBDA scores correlated with CRP (r = 0.755, P < 0.001), but were often discordant, being moderate or high for 19%, 55% and 87% of patients with CRP ⩽0.1, 0.1 to ⩽0.3, or 0.3 to ⩽1.0 mg/dl, respectively. Among patients with CRP ⩽1.0 mg/dl, swollen joint count (SJC) increased linearly across levels of MBDA score, both with (P = 0.021) and without (P = 0.004) adjustment for CRP, whereas CRP was not associated with SJC. The 28-joint-DAS-CRP, other composite measures, and their non-joint-count component measures were significantly greater for patients with RA and FM (n = 25) versus RA alone (n = 173) (all P ⩽ 0.005). MBDA scores and CRP were similar between groups.
MBDA scores frequently indicated RA disease activity when CRP did not. Neither one was significantly greater among patients with RA and FM versus RA alone. Thus, MBDA score may be a useful objective measure for identifying RA patients with active inflammation when CRP is low (⩽1.0 mg/dl), including RA patients with concomitant FM.
研究伴有或不伴有纤维肌痛(FM)的类风湿关节炎(RA)患者中,多生物标志物疾病活动度(MBDA)评分、C反应蛋白(CRP)与临床疾病活动度指标之间的关联。
在一个确诊RA患者的观察性队列中,我们通过等级相关和交叉分类对MBDA评分与CRP进行了横断面分析。通过单因素和多因素分析,比较了单纯RA患者与合并FM的RA患者(RA合并FM)之间的MBDA评分、CRP及疾病活动度的临床指标。
198例患者中有184例(93%)的CRP≤1.0mg/dl。MBDA评分与CRP相关(r = 0.755,P < 0.001),但二者常不一致,CRP≤0.1mg/dl、0.1至≤0.3mg/dl或0.3至≤1.0mg/dl的患者中,分别有19%、55%和87%的患者MBDA评分为中度或高度。在CRP≤1.0mg/dl的患者中,无论是否对CRP进行校正,肿胀关节计数(SJC)均随MBDA评分水平呈线性增加(校正后P = 0.021,未校正P = 0.004),而CRP与SJC无关。与单纯RA患者(n = 173)相比,RA合并FM患者(n = 25)的28关节疾病活动评分- CRP(DAS28-CRP)、其他综合指标及其非关节计数组成指标均显著更高(所有P≤0.005)。两组间MBDA评分和CRP相似。
当CRP未显示RA疾病活动时,MBDA评分常可显示。RA合并FM患者与单纯RA患者相比,二者均无显著更高。因此,当CRP较低(≤1.0mg/dl)时,MBDA评分可能是识别有活动性炎症的RA患者的有用客观指标,包括合并FM的RA患者。