Martin Natasha K, Vickerman Peter, Brew Iain F, Williamson Joan, Miners Alec, Irving William L, Saksena Sushma, Hutchinson Sharon J, Mandal Sema, O'Moore Eamonn, Hickman Matthew
Division of Global Public Health, University of California San Diego, San Diego, CA.
School of Social and Community Medicine, University of Bristol, Bristol, UK.
Hepatology. 2016 Jun;63(6):1796-808. doi: 10.1002/hep.28497. Epub 2016 Mar 22.
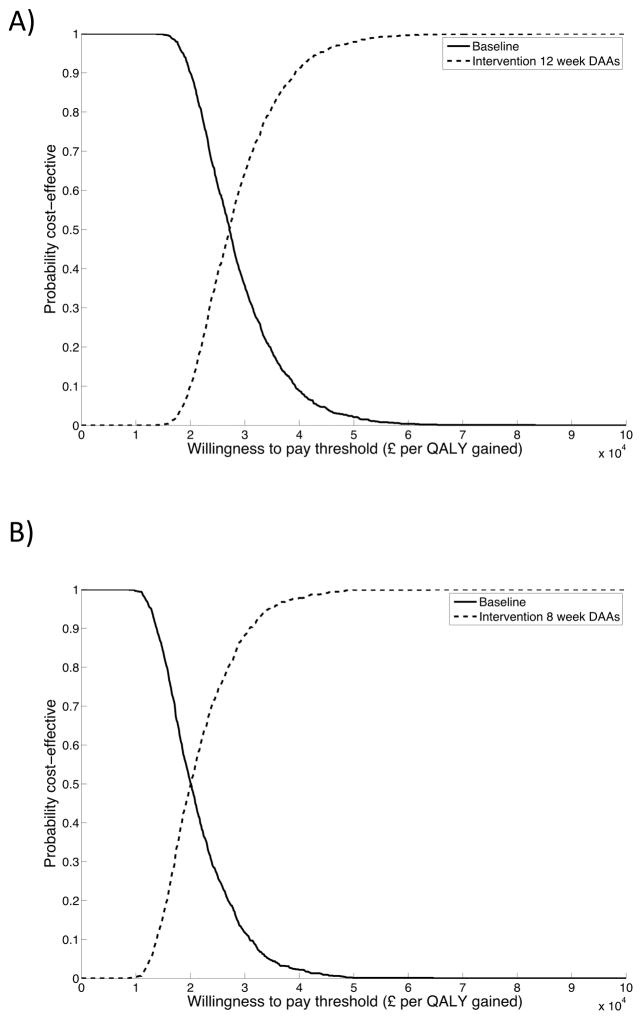
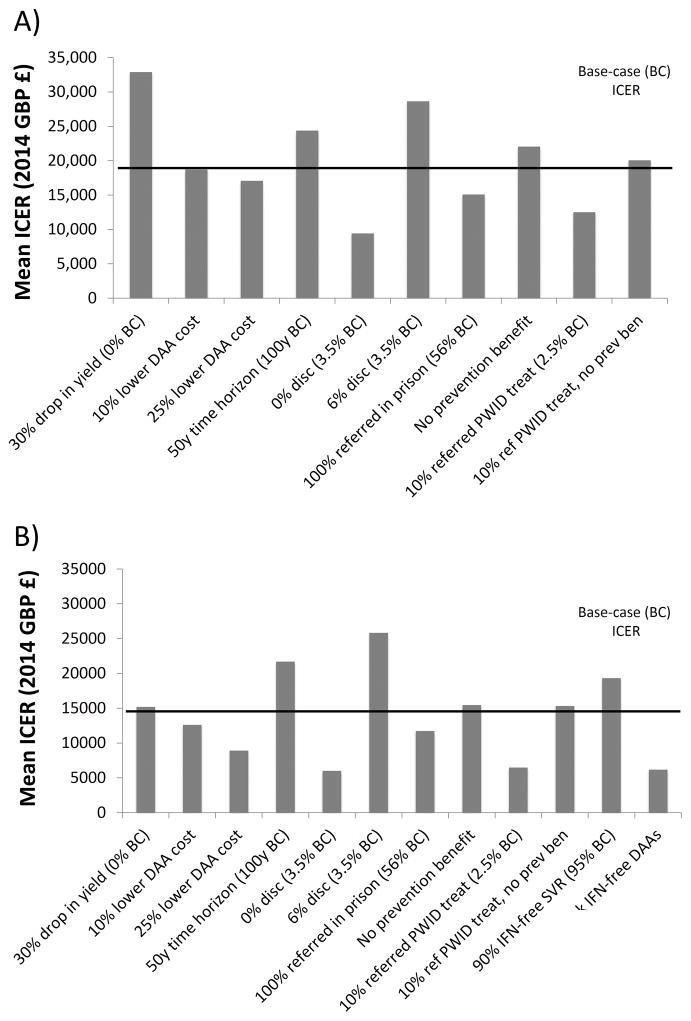
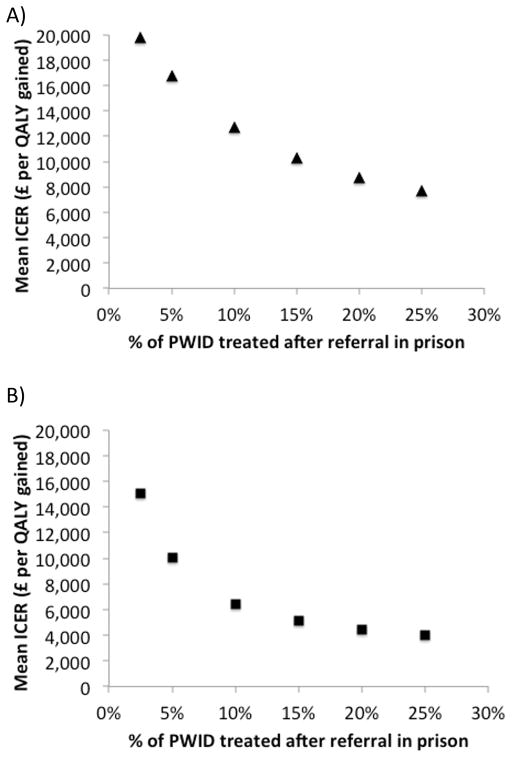
Prisoners have a high prevalence of hepatitis C virus (HCV), but case-finding may not have been cost-effective because treatment often exceeded average prison stay combined with a lack of continuity of care. We assessed the cost-effectiveness of increased HCV case-finding and treatment in UK prisons using short-course therapies. A dynamic HCV transmission model assesses the cost-effectiveness of doubling HCV case-finding (achieved through introducing opt-out HCV testing in UK pilot prisons) and increasing treatment in UK prisons compared to status quo voluntary risk-based testing (6% prison entrants/year), using currently recommended therapies (8-24 weeks) or interferon (IFN)-free direct-acting antivirals (DAAs; 8-12 weeks, 95% sustained virological response, £3300/week). Costs (British pounds, £) and health utilities (quality-adjusted life years) were used to calculate mean incremental cost-effectiveness ratios (ICERs). We assumed 56% referral and 2.5%/25% of referred people who inject drugs (PWID)/ex-PWID treated within 2 months of diagnosis in prison. PWID and ex-PWID or non-PWID are in prison an average 4 and 8 months, respectively. Doubling prison testing rates with existing treatments produces a mean ICER of £19,850/quality-adjusted life years gained compared to current testing/treatment and is 45% likely to be cost-effective under a £20,000 willingness-to-pay threshold. Switching to 8-week to 12-week IFN-free DAAs in prisons could increase cost-effectiveness (ICER £15,090/quality-adjusted life years gained). Excluding prevention benefit decreases cost-effectiveness. If >10% referred PWID are treated in prison (2.5% base case), either treatment could be highly cost-effective (ICER<£13,000). HCV case-finding and IFN-free DAAs could be highly cost-effective if DAA cost is 10% lower or with 8 weeks' duration.
Increased HCV testing in UK prisons (such as through opt-out testing) is borderline cost-effective compared to status quo voluntary risk-based testing under a £20,000 willingness to pay with current treatments but likely to be cost-effective if short-course IFN-free DAAs are used and could be highly cost-effective if PWID treatment rates were increased. (Hepatology 2016;63:1796-1808).
丙型肝炎病毒(HCV)在囚犯中的患病率很高,但病例发现可能并不具有成本效益,因为治疗时间往往超过平均刑期,且缺乏连续护理。我们评估了在英国监狱中使用短程疗法增加HCV病例发现和治疗的成本效益。一个动态HCV传播模型评估了将HCV病例发现率翻倍(通过在英国试点监狱引入退出式HCV检测实现)以及与现状基于风险的自愿检测(每年6%的入狱者)相比增加英国监狱治疗的成本效益,使用当前推荐的疗法(8 - 24周)或不含干扰素(IFN)的直接作用抗病毒药物(DAAs;8 - 12周,持续病毒学应答率95%,每周3300英镑)。成本(英镑,£)和健康效用(质量调整生命年)用于计算平均增量成本效益比(ICERs)。我们假设在监狱诊断后2个月内有56%的转诊率,以及2.5%/25%的注射毒品者(PWID)/曾注射毒品者(ex - PWID)接受治疗。PWID和ex - PWID或非PWID在监狱的平均服刑时间分别为4个月和8个月。与当前检测/治疗相比,在现有治疗基础上使监狱检测率翻倍,每获得一个质量调整生命年的平均ICER为19,850英镑,在支付意愿阈值为20,000英镑的情况下,有45%的可能性具有成本效益。在监狱中改用8至12周的不含IFN的DAAs可提高成本效益(ICER为每获得一个质量调整生命年15,090英镑)。排除预防效益会降低成本效益。如果在监狱中接受治疗的转诊PWID比例超过10%(基础病例为2.5%),则两种治疗方法都可能具有很高的成本效益(ICER<13,000英镑)。如果DAA成本降低10%或疗程为8周,HCV病例发现和不含IFN的DAAs可能具有很高的成本效益。
在支付意愿为20,000英镑的情况下,与现状基于风险的自愿检测相比,在英国监狱中增加HCV检测(如通过退出式检测)在使用当前治疗方法时成本效益处于临界状态,但如果使用短程不含IFN的DAAs则可能具有成本效益,如果提高PWID的治疗率则可能具有很高的成本效益。(《肝病学》2016年;63卷:1796 - 1808页)