Smith J K, Marciani L, Humes D J, Francis S T, Gowland P, Spiller R C
Nottingham Digestive Diseases Centre, School of Medicine, University of Nottingham, Nottingham, UK.
Sir Peter Mansfield Magnetic Resonance Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, UK.
Neurogastroenterol Motil. 2016 Jun;28(6):900-13. doi: 10.1111/nmo.12790. Epub 2016 Mar 11.
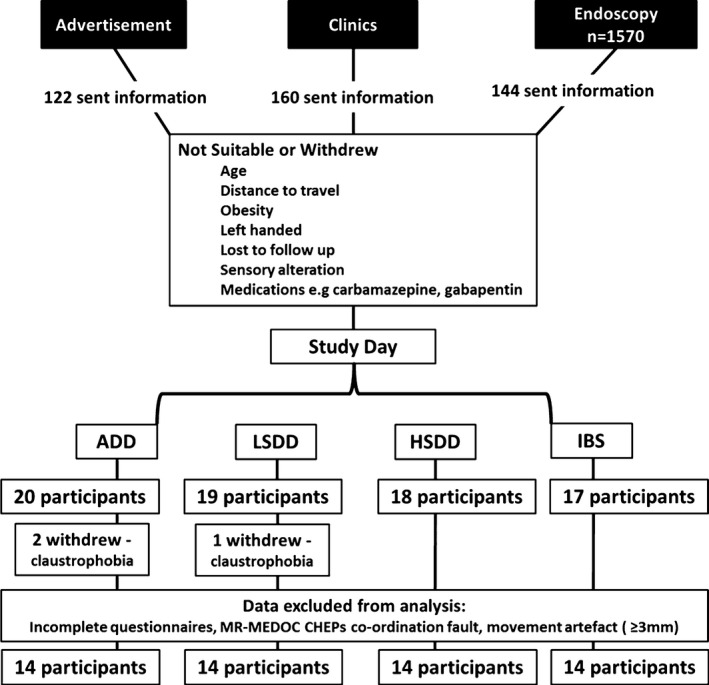
The relative importance of peripheral nerve injury or central pain processing in painful diverticular disease (DD) is unclear. Functional magnetic resonance imaging (fMRI) has demonstrated that dysfunctional central pain processing predominates in irritable bowel syndrome (IBS). This study aims to identify anticipatory changes in symptomatic DD (SDD) compared to asymptomatic DD (ADD) and IBS patients.
Gastrointestinal symptoms and somatization were evaluated via the Patient Health Question-12 Somatic Symptom and the SDD group divided into low (≤6 [LSDD]) and high (≥7 [HSDD]) somatization. Cued painful cutaneous thermal stimuli were delivered to the left hand and foot during fMRI. Fixed effect group analysis of the 'cued' anticipatory phase was performed.
Within the right posterior insula, greater deactivation was found in the ADD compared to other groups. In emotion processing centers, anterior and middle insula, greater activation was identified in all patient compared to the ADD group, and in LSDD compared to IBS and HSDD groups. In comparison, amygdala deactivation was greater in ADD than the IBS and HSDD groups, and in LSDD vs HSDD groups. Descending nociceptive control centers, such as the superior medial frontal and orbitofrontal cortex, also showed greater deactivation in the ADD and LSDD compared to the HSDD and IBS groups.
CONCLUSIONS & INFERENCES: The HSDD group have altered anticipatory responses to thermal pain, similar to IBS group. The LSDD are similar to ADD group. This suggests underlying differences in pain pathophysiology, and the need for individualized treatment strategies to target the cause of their chronic pain.
在疼痛性憩室病(DD)中,周围神经损伤或中枢性疼痛处理的相对重要性尚不清楚。功能磁共振成像(fMRI)已表明,在肠易激综合征(IBS)中,功能失调的中枢性疼痛处理占主导地位。本研究旨在确定有症状的DD(SDD)与无症状的DD(ADD)及IBS患者相比的预期变化。
通过患者健康问卷-12躯体症状评估胃肠道症状和躯体化情况,并将SDD组分为低躯体化(≤6 [LSDD])和高躯体化(≥7 [HSDD])。在fMRI期间,对左手和左脚施加提示性疼痛性皮肤热刺激。对“提示性”预期阶段进行固定效应组分析。
在右后岛叶,ADD组与其他组相比发现更大程度的失活。在情绪处理中心,即前岛叶和中岛叶,所有患者组与ADD组相比有更大程度的激活,LSDD组与IBS组和HSDD组相比有更大程度的激活。相比之下,杏仁核失活在ADD组比IBS组和HSDD组更明显,在LSDD组与HSDD组相比也更明显。下行伤害性控制中心,如内侧额上回和眶额皮质,与HSDD组和IBS组相比,在ADD组和LSDD组也显示出更大程度的失活。
HSDD组对热痛的预期反应发生改变,与IBS组相似。LSDD组与ADD组相似。这表明疼痛病理生理学存在潜在差异,需要针对其慢性疼痛原因制定个体化治疗策略。