Altshuler Lisa, Plaksin Joseph, Zabar Sondra, Wallach Andrew, Sawicki Chester, Kundrod Sarita, Kalet Adina
Program on Medical Education, Innovations and Research (PrMEIR), Division of General Internal Medicine and Clinical Innovation, New York University School of Medicine, New York, NY, United States.
JMIR Res Protoc. 2016 Apr 21;5(2):e68. doi: 10.2196/resprot.5376.
In the patient-centered medical home model of health care, both health care providers (HCPs) and patients must understand their respective roles and responsibilities, view the other as a partner, and use communication skills that promote shared decision making. This is particularly necessary in chronic conditions where outcomes depend on behavior change and in underserved populations where the burden of chronic disease is high.
The objectives of this study are to determine if a Patient Empowerment Program (PEP) (1) is acceptable to patients and feasible across multiple clinical sites; (2) will increase patient preference for control in medical decision making, improve patient perceptions of patient-HCP communication, and increase patient activation; (3) is associated with an increase in diabetes self-management behaviors; and (4) has an effect on hemoglobin A1c (HbA1c) level.
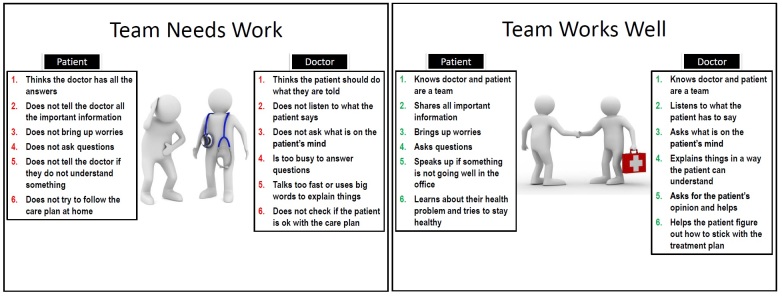
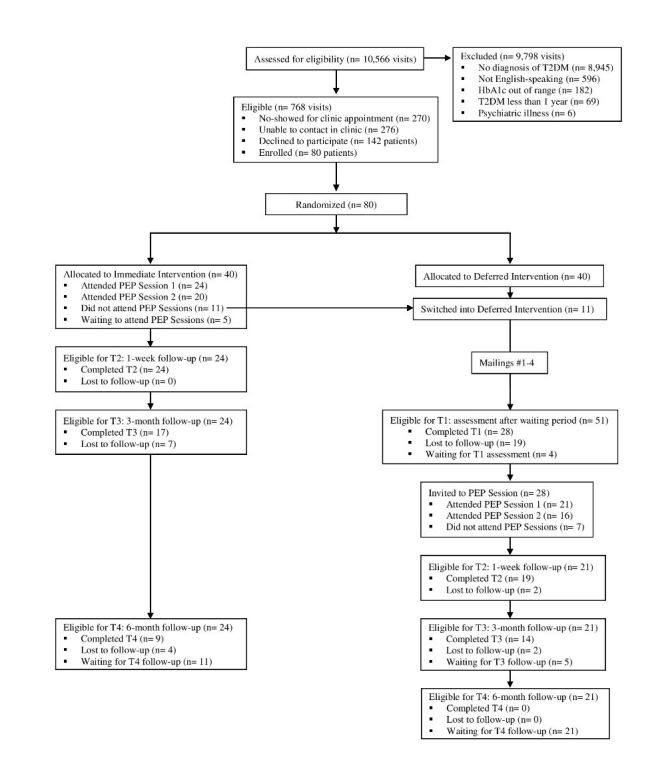
This study recruited English-speaking adult patients with type 2 diabetes mellitus from three urban clinical sites in New York City and randomized them to an immediate intervention group that completed the PEP intervention or a deferred intervention group that served as a wait-list control and completed the PEP intervention after 3-4 months. The PEP intervention consists of two facilitated small group sessions. Session 1 focuses on defining HCP and patient roles in the medical encounter by introducing ideal communication behaviors in each role and by providing both positive and negative examples of patient-HCP encounters. Session 2 focuses on practicing communication skills by role-playing with actors who serve as standardized health care providers. After the role play, participants set goals for their own health care and for future interactions with their HCPs. Outcome measures include the Patient Activation Measure; Ask, Understand, Remember Assessment; Krantz Health Opinion Survey; SF-12v2 Health Survey; Diabetes Self-Management Questionnaire; and HbA1c. These measures will be assessed at the time of enrollment, after the waiting period (deferred intervention only), and then postintervention at 1 week, 3 months, and 6 months.
Study recruitment occurred from November 2014 to June 2015, with a total of 80 patients enrolled. To date, 45 participants have attended at least one session of the PEP intervention. Further intervention sessions and post-intervention follow-up are ongoing, with data collection set to be completed in April 2016 and results of data analysis available by June 2016.
From preliminary participant self-report data, our PEP intervention is acceptable to low-income, low-health literate patients and feasible to hold across multiple clinical sites. Participants have reported learning specific ways to change their behaviors at their next HCP visit (eg, stating their opinions, asking more questions). With the forthcoming quantitative data on participant attitudinal and behavior change, the PEP intervention may ultimately empower participants within the medical encounter and improve health outcomes.
在以患者为中心的医疗家庭保健模式中,医疗保健提供者(HCPs)和患者都必须了解各自的角色和责任,将对方视为合作伙伴,并运用促进共同决策的沟通技巧。这在慢性病(其治疗结果取决于行为改变)以及慢性病负担较高的服务不足人群中尤为必要。
本研究的目的是确定患者赋权计划(PEP)(1)是否为患者所接受且在多个临床场所可行;(2)是否会增加患者在医疗决策中对控制权的偏好,改善患者对医患沟通的认知,并提高患者的积极性;(3)是否与糖尿病自我管理行为的增加相关;以及(4)对糖化血红蛋白(HbA1c)水平是否有影响。
本研究从纽约市的三个城市临床场所招募了讲英语的成年2型糖尿病患者,并将他们随机分为立即干预组(完成PEP干预)或延迟干预组(作为等待名单对照,在3 - 4个月后完成PEP干预)。PEP干预包括两次有指导的小组会议。第一次会议通过介绍每个角色中的理想沟通行为以及提供医患互动的正面和负面例子,重点在于明确医疗互动中HCP和患者的角色。第二次会议通过与充当标准化医疗保健提供者的演员进行角色扮演来练习沟通技巧。角色扮演后,参与者为自己的医疗保健以及未来与HCP的互动设定目标。结果测量包括患者积极性测量;询问、理解、记忆评估;克兰茨健康意见调查;SF - 12v2健康调查;糖尿病自我管理问卷;以及HbA1c。这些测量将在入组时、等待期后(仅延迟干预组)以及干预后1周、3个月和6个月进行评估。
研究招募工作于2014年11月至2015年6月进行,共有80名患者入组。迄今为止,45名参与者至少参加了一次PEP干预会议。进一步的干预会议和干预后随访正在进行中,数据收集定于2016年4月完成,数据分析结果将于2016年6月可得。
根据初步的参与者自我报告数据,我们的PEP干预对于低收入、健康素养低的患者是可接受的,并且在多个临床场所开展是可行的。参与者报告称学到了在下一次看HCP时改变行为的具体方法(例如,表达自己的意见、多提问)。随着即将获得的关于参与者态度和行为改变的定量数据,PEP干预最终可能会在医疗互动中增强参与者的能力并改善健康结果。