Donneyong Macarius M, Bykov Katsiaryna, Bosco-Levy Pauline, Dong Yaa-Hui, Levin Raisa, Gagne Joshua J
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA 02120.
Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA 02120 Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, USA 02115.
BMJ. 2016 Sep 30;354:i5014. doi: 10.1136/bmj.i5014.
To compare differences in mortality between women concomitantly treated with tamoxifen and selective serotonin reuptake inhibitors (SSRIs) that are potent inhibitors of the cytochrome-P450 2D6 enzyme (CYP2D6) versus tamoxifen and other SSRIs.
Population based cohort study.
Five US databases covering individuals enrolled in private and public health insurance programs from 1995 to 2013.
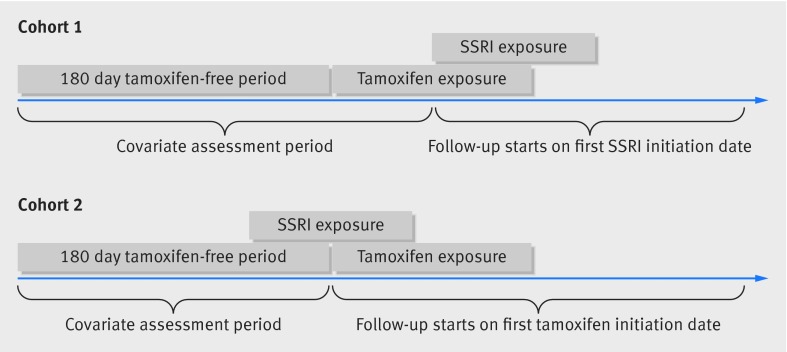
Two cohorts of women who started taking tamoxifen. In cohort 1, women started taking an SSRI during tamoxifen treatment. In cohort 2, women were already taking an SSRI when they started taking tamoxifen.
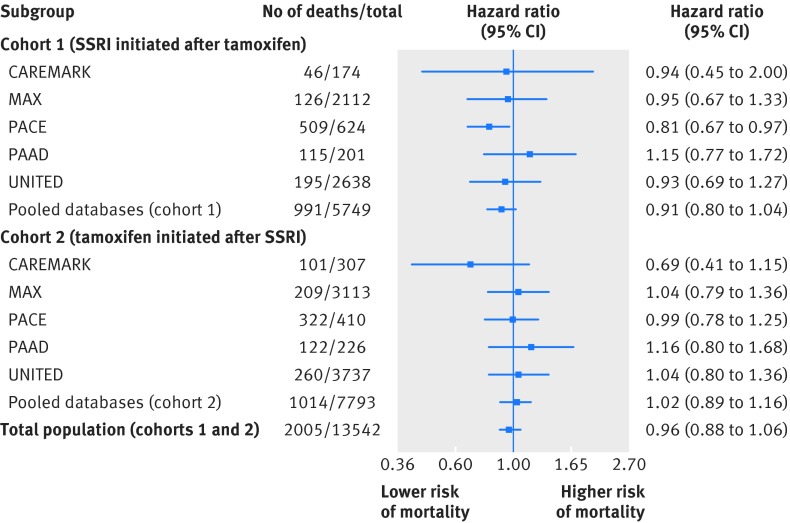
All cause mortality in each cohort in women taking SSRIs that are potent inhibitors of CYP2D6 (paroxetine, fluoxetine) versus other SSRIs. Propensity scores were used to match exposure groups in a variable ratio fashion. Results were measured separately for each cohort and combined hazard ratios calculated from Cox regression models across the two cohorts with random effects meta-analysis.
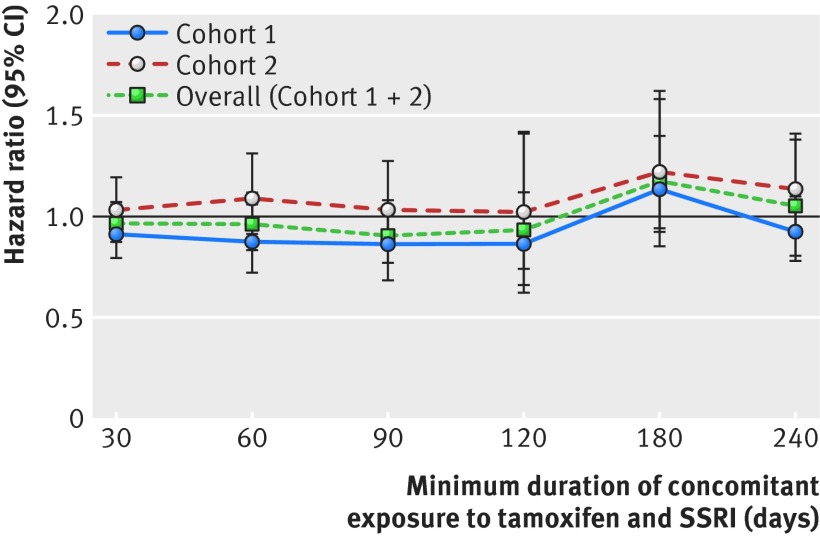
There were 6067 and 8465 new users of tamoxifen in cohorts 1 and 2, respectively. Mean age was 55. A total of 991 and 1014 deaths occurred in cohorts 1 and 2 during a median follow-up of 2.2 (interquartile range 0.9-4.5) and 2.0 (0.8-3.9) years, respectively. The pooled hazard ratio for death for potent inhibitors (rate 58.6/1000 person years) compared with other SSRIs (rate 57.9/1000 person years) across cohorts 1 and 2 was 0.96 (95% confidence interval 0.88 to 1.06). Results were consistent across sensitivity analyses.
Concomitant use of tamoxifen and potent CYP2D6 inhibiting SSRIs versus other SSRIs was not associated with an increased risk of death.
比较同时接受他莫昔芬与细胞色素P450 2D6酶(CYP2D6)强效抑制剂选择性5-羟色胺再摄取抑制剂(SSRI)治疗的女性与接受他莫昔芬和其他SSRI治疗的女性之间的死亡率差异。
基于人群的队列研究。
五个美国数据库,涵盖1995年至2013年参加私人和公共医疗保险计划的个体。
两组开始服用他莫昔芬的女性。在队列1中,女性在他莫昔芬治疗期间开始服用SSRI。在队列2中,女性在开始服用他莫昔芬时已经在服用SSRI。
服用CYP2D6强效抑制剂(帕罗西汀、氟西汀)的SSRI的女性与服用其他SSRI的女性在每个队列中的全因死亡率。倾向评分用于以可变比例方式匹配暴露组。对每个队列分别测量结果,并通过随机效应荟萃分析从两个队列的Cox回归模型计算合并风险比。
队列1和队列2中分别有6067名和8465名他莫昔芬新使用者。平均年龄为55岁。在队列1和队列2中,分别在中位随访2.2年(四分位间距0.9 - 4.5)和2.0年(0.8 - 3.9)期间发生了991例和1014例死亡。队列1和队列2中,强效抑制剂(发生率58.6/1000人年)与其他SSRI(发生率57.9/1000人年)相比的合并死亡风险比为0.96(95%置信区间0.88至1.06)。敏感性分析结果一致。
同时使用他莫昔芬与强效CYP2D6抑制性SSRI和其他SSRI相比,死亡风险并未增加。