Yoon Ho Il, Kwon Oh-Ran, Kang Kyung Nam, Shin Yong Sung, Shin Ho Sang, Yeon Eun Hee, Kwon Keon Young, Hwang Ilseon, Jeon Yoon Kyung, Kim Yongdai, Kim Chul Woo
Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
BioInfra, Inc., Seoul, Korea.
J Cancer Prev. 2016 Sep;21(3):187-193. doi: 10.15430/JCP.2016.21.3.187. Epub 2016 Sep 30.
Despite major advances in lung cancer treatment, early detection remains the most promising way of improving outcomes. To detect lung cancer in earlier stages, many serum biomarkers have been tested. Unfortunately, no single biomarker can reliably detect lung cancer. We combined a set of 2 tumor markers and 4 inflammatory or metabolic markers and tried to validate the diagnostic performance in lung cancer.
We collected serum samples from 355 lung cancer patients and 590 control subjects and divided them into training and validation datasets. After measuring serum levels of 6 biomarkers (human epididymis secretory protein 4 [HE4], carcinoembryonic antigen [CEA], regulated on activation, normal T cell expressed and secreted [RANTES], apolipoprotein A2 [ApoA2], transthyretin [TTR], and secretory vascular cell adhesion molecule-1 [sVCAM-1]), we tested various sets of biomarkers for their diagnostic performance in lung cancer.
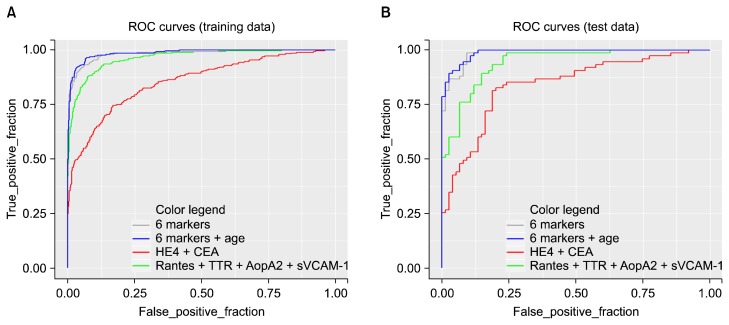
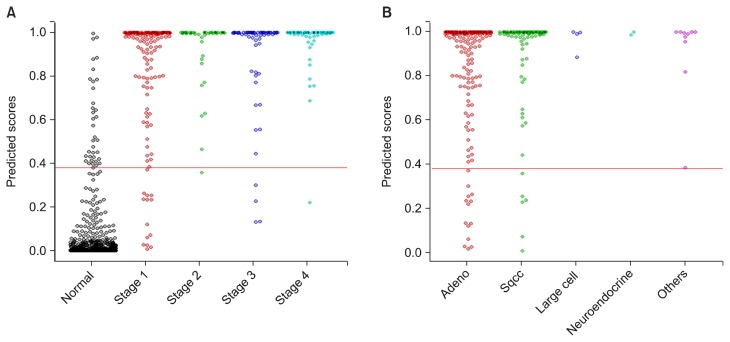
In a training dataset, the area under the curve (AUC) values were 0.821 for HE4, 0.753 for CEA, 0.858 for RANTES, 0.867 for ApoA2, 0.830 for TTR, and 0.552 for sVCAM-1. A model using all 6 biomarkers and age yielded an AUC value of 0.986 and sensitivity of 93.2% (cutoff at specificity 94%). Applying this model to the validation dataset showed similar results. The AUC value of the model was 0.988, with sensitivity of 93.33% and specificity of 92.00% at the same cutoff point used in the validation dataset. Analyses by stages and histologic subtypes all yielded similar results.
Combining multiple tumor and systemic inflammatory markers proved to be a valid strategy in the diagnosis of lung cancer.
尽管肺癌治疗取得了重大进展,但早期检测仍然是改善预后最有前景的方法。为了在更早期阶段检测肺癌,人们对多种血清生物标志物进行了测试。遗憾的是,没有单一生物标志物能够可靠地检测肺癌。我们将一组2种肿瘤标志物和4种炎症或代谢标志物相结合,试图验证其在肺癌诊断中的性能。
我们收集了355例肺癌患者和590例对照受试者的血清样本,并将其分为训练数据集和验证数据集。在测量6种生物标志物(人附睾分泌蛋白4[HE4]、癌胚抗原[CEA]、活化调节正常T细胞表达和分泌因子[RANTES]、载脂蛋白A2[ApoA2]、转甲状腺素蛋白[TTR]和分泌型血管细胞黏附分子-1[sVCAM-1])的血清水平后,我们测试了各种生物标志物组合在肺癌诊断中的性能。
在训练数据集中,HE4的曲线下面积(AUC)值为0.821,CEA为0.753,RANTES为0.858,ApoA2为0.867,TTR为0.830,sVCAM-1为0.552。使用所有6种生物标志物和年龄构建的模型AUC值为0.986,敏感性为93.2%(特异性截止值为94%)。将该模型应用于验证数据集显示了相似的结果。该模型在验证数据集中使用的相同截止点下,AUC值为0.988,敏感性为93.33%,特异性为92.00%。按阶段和组织学亚型分析均得出相似结果。
结合多种肿瘤和全身炎症标志物被证明是诊断肺癌的有效策略。