Makam Raghavendra Charan P, Erskine Nathaniel, McManus David D, Lessard Darleen, Gore Joel M, Yarzebski Jorge, Goldberg Robert J
Department of Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, Massachusetts.
Department of Medicine, University of Massachusetts Medical School, Worcester, Massachusetts.
Am J Cardiol. 2016 Dec 15;118(12):1792-1797. doi: 10.1016/j.amjcard.2016.08.065. Epub 2016 Sep 13.
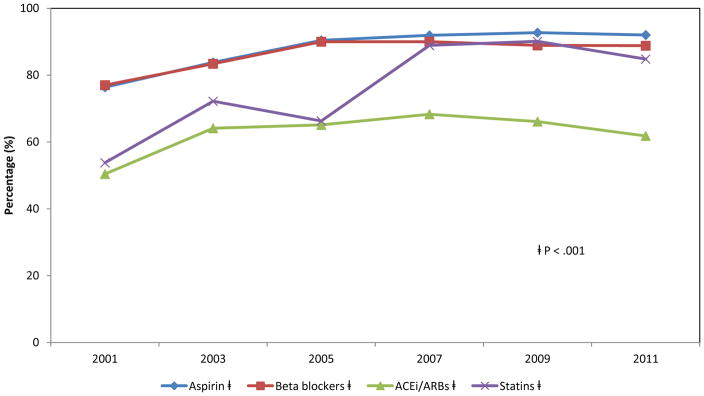
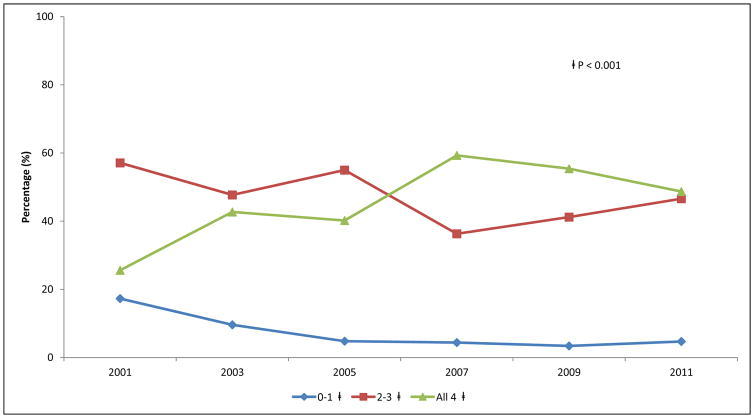
Optimization of medical therapy during discharge planning is vital for improving patient outcomes after hospitalization for acute myocardial infarction (AMI). However, limited information is available about recent trends in the prescribing of evidence-based medical therapies in these patients, especially from a population-based perspective. We describe decade-long trends in the discharge prescribing of aspirin, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, β blockers, and statins in hospital survivors of AMI. The study population consisted of 5,253 patients who were discharged from all 11 hospitals in central Massachusetts after AMI in 6 biennial periods from 2001 to 2011. Combination medical therapy (CMT) was defined as the prescription of all 4 cardiac medications at hospital discharge. The average age of this patient population was 69.2 years and 57.7% were men. Significant increases were observed in the use of CMT, from 25.6% in 2001 to 48.7% in 2011, with increases noted for each of the individual cardiac medications examined. Subgroup analysis also showed improvement in discharge prescriptions for P2Y12 inhibitors in patients who underwent a percutaneous coronary intervention. Presence of a do-not-resuscitate order, before co-morbidities, hospitalization for non-ST-segment elevation myocardial infarction, admission to a nonteaching hospital, and failure to undergo cardiac catheterization or a percutaneous coronary intervention were associated with underuse of CMT. In conclusion, our study demonstrates encouraging trends in the prescribing of evidence-based medications at hospital discharge for AMI. However, certain patient subgroups continue to be at risk for underuse of CMT, suggesting the need for strategies to enhance compliance with current practice guidelines.
在急性心肌梗死(AMI)患者出院计划期间优化药物治疗对于改善其出院后的预后至关重要。然而,关于这些患者循证药物治疗处方的近期趋势,尤其是基于人群视角的信息有限。我们描述了AMI住院幸存者出院时阿司匹林、血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂、β受体阻滞剂和他汀类药物处方的十年趋势。研究人群包括2001年至2011年期间6个双年度从马萨诸塞州中部所有11家医院出院的5253例AMI患者。联合药物治疗(CMT)定义为出院时开具所有4种心脏药物。该患者群体的平均年龄为69.2岁,男性占57.7%。观察到CMT的使用显著增加,从2001年的25.6%增至2011年的48.7%,所检查的每种心脏药物的使用均有增加。亚组分析还显示,接受经皮冠状动脉介入治疗的患者中P2Y12抑制剂的出院处方有所改善。存在不进行心肺复苏医嘱、有合并症、非ST段抬高型心肌梗死住院、入住非教学医院以及未接受心导管检查或经皮冠状动脉介入治疗与CMT使用不足相关。总之,我们的研究表明AMI患者出院时循证药物处方呈现令人鼓舞的趋势。然而,某些患者亚组仍有CMT使用不足的风险,这表明需要采取策略以提高对现行实践指南的依从性。