Tumor Vaccine Group, Center for Translational Medicine in Women's Health, University of Washington, 850 Republican Street, 2nd Floor, Box 358050, Seattle, WA 98195-8050 USA.
J Immunother Cancer. 2016 Oct 18;4:59. doi: 10.1186/s40425-016-0165-6. eCollection 2016.
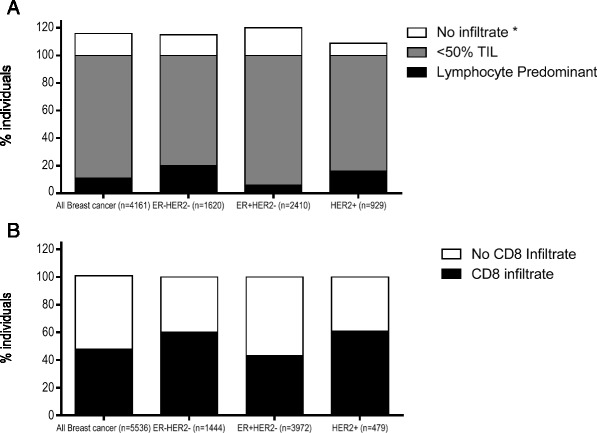
Tumor infiltrating lymphocytes (TIL) play an essential role in mediating response to chemotherapy and improving clinical outcomes in all subtypes of breast cancer. Triple negative breast cancers (TN) are most likely to have tumors with >50 % lymphocytic infiltrate, termed lymphocyte predominant breast cancer, and derive the greatest survival benefit from each 10 % increase in TIL. The majority of HER2 breast cancers have similar level of immune infiltrate as TN breast cancer yet the presence of TILs has not shown the same survival benefit. For HER2 breast cancers, type 1 T-cells, either increased TBET tumor infiltration or increased type 1 HER2-specific CD4 T-cells in the peripheral blood, are associated with better outcomes. Hormone receptor positive HER2 negative tumors tend to have the least immune infiltrate yet are the only breast cancer subtype to show worse prognosis with increased FOXP3 regulatory T-cell infiltrate. Notably, all breast cancer subtypes have tumors with low, intermediate, or high TIL infiltrate. Tumors with high TILs may also have increased PD-L1 expression which might be the reason that TN breast cancer seems to demonstrate the most robust clinical response to immune checkpoint inhibitor therapy but further investigation is needed. Tumors with intermediate or low levels of pre-treatment immune infiltrate, on the other hand, may benefit from an intervention that may increase TIL, particularly type 1 T-cells. Examples of these interventions include specific types of cytotoxic chemotherapy, radiation, or vaccine therapy. Therefore, the systematic evaluation of TIL and specific populations of TIL may be able to both guide prognosis and the appropriate sequencing of therapies in breast cancer.
肿瘤浸润淋巴细胞 (TIL) 在介导对化疗的反应和改善所有乳腺癌亚型的临床结果方面发挥着重要作用。三阴性乳腺癌 (TN) 最有可能具有 >50%淋巴细胞浸润的肿瘤,称为淋巴细胞为主型乳腺癌,并且 TIL 每增加 10%就会获得最大的生存获益。大多数 HER2 乳腺癌的免疫浸润程度与 TN 乳腺癌相似,但 TIL 的存在并未显示出相同的生存获益。对于 HER2 乳腺癌,1 型 T 细胞,无论是增加 TBET 肿瘤浸润,还是增加外周血中 1 型 HER2 特异性 CD4 T 细胞,都与更好的结果相关。激素受体阳性 HER2 阴性肿瘤的免疫浸润程度往往最低,但却是唯一一种随着 FOXP3 调节性 T 细胞浸润增加而预后恶化的乳腺癌亚型。值得注意的是,所有乳腺癌亚型的肿瘤都有低、中或高 TIL 浸润。高 TIL 浸润的肿瘤也可能增加 PD-L1 表达,这可能是 TN 乳腺癌似乎对免疫检查点抑制剂治疗表现出最强大临床反应的原因,但需要进一步研究。另一方面,具有中等或低水平预处理免疫浸润的肿瘤可能受益于可能增加 TIL 的干预措施,特别是 1 型 T 细胞。这些干预措施的例子包括特定类型的细胞毒性化疗、放疗或疫苗治疗。因此,对 TIL 和 TIL 的特定群体进行系统评估,可能既能够指导预后,又能够指导乳腺癌治疗的适当顺序。