Yamada Yoshiya, Katsoulakis Evangelia, Laufer Ilya, Lovelock Michael, Barzilai Ori, McLaughlin Lily A, Zhang Zhigang, Schmitt Adam M, Higginson Daniel S, Lis Eric, Zelefsky Michael J, Mechalakos James, Bilsky Mark H
Departments of1Radiation Oncology.
2Neurological Surgery.
Neurosurg Focus. 2017 Jan;42(1):E6. doi: 10.3171/2016.9.FOCUS16369.
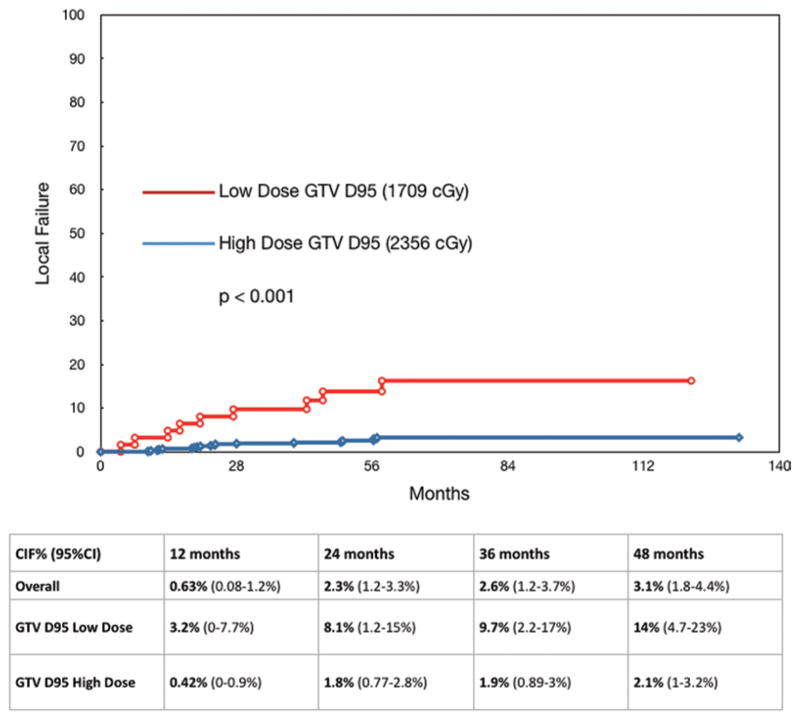
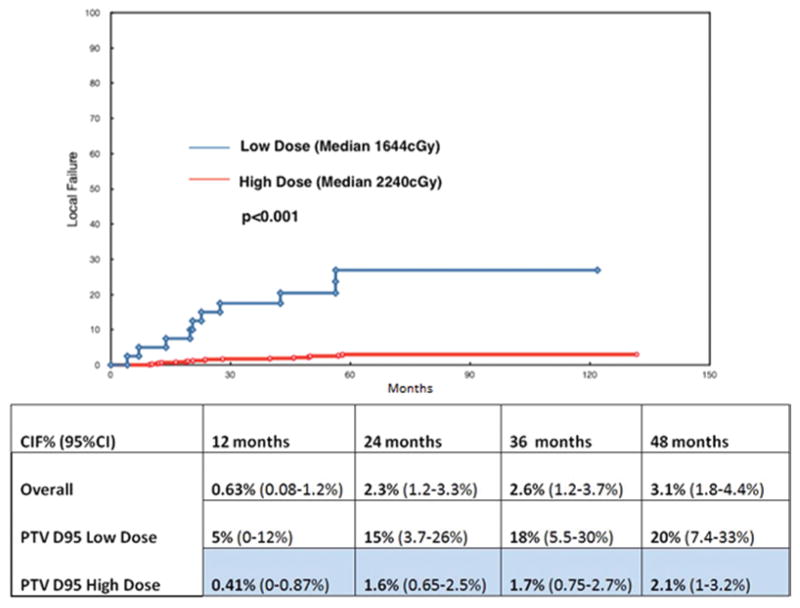
OBJECTIVE An analysis of factors contributing to durable radiographic control of spinal metastases was undertaken, drawing from a large single-institution database in an attempt to elucidate indications and dose requirements for successful treatment. METHODS All patients treated at a single institution with stereotactic radiosurgery (SRS) of the spine as first-line therapy were assessed for local progression of the treated site, defined as radiographic enlargement of the treated tumor and/or biopsy-proven evidence of active tumor cells. All patients were followed with CT, PET, or MR imaging every 3-6 months until death. Treatment decisions were made by a multidisciplinary team of radiation oncologists, neurosurgeons, and neuroradiologists. Target volumes were defined according to the international consensus guidelines and were reviewed in a multidisciplinary conference. Image-guided techniques and intensity modulation were used for every case. The tumor's histological type, gross tumor volume (GTV), dose that covers 95% of the GTV (GTV D95), percentage of GTV covered by 95% of the prescribed dose (GTV V95), planning target volume (PTV), dose that covers 95% of the PTV (PTV D95), and percentage of PTV covered by 95% of the prescribed dose (PTV V95) were analyzed for significance in relation to local control, based on time to local progression. RESULTS A total of 811 lesions were treated in 657 patients between 2003 and 2015 at a single institution. The mean follow-up and overall survival for the entire cohort was 26.9 months (range 2-141 months). A total of 28 lesions progressed and the mean time to failure was 26 months (range 9.7-57 months). The median prescribed dose was 2400 cGy (range 1600-2600 cGy). Both GTV D95 and PTV D95 were highly significantly associated with local failure in univariate analysis, but GTV and PTV and histological type did not reach statistical significance. The median GTV D95 for the cohort equal to or above the GTV D95 1830 cGy cut point (high dose) was 2356 cGy, and it was 1709 cGy for the cohort of patients who received less than 1830 cGy (low dose). In terms of PTV D95, the median dose for those equal to or above the cut point of 1740 cGy (high dose) was 2233 cGy, versus 1644 cGy for those lesions below the PTV D95 cut point of 1740 cGy (low dose). CONCLUSIONS High-dose single-session SRS provides durable long-term control, regardless of the histological findings or tumor size. In this analysis, the only significant factors predictive of local control were related to the actual dose of radiation given. Although the target volumes were well treated with the intended dose, those lesions irradiated to higher doses (median GTV D95 2356 cGy, minimum 1830 cGy) had a significantly higher probability of durable local control than those treated with lower doses (median PTV D95 2232 cGy, minimum of 1740 cGy) (p < 0.001). Patients in the high-dose cohort had a 2% cumulative rate of local failure. Histological findings were not associated with local failure, suggesting that radioresistant histological types benefit in particular from radiosurgery. For patients with a favorable prognosis, a higher dose of SRS is important for long-term outcomes.
从一个大型单机构数据库中分析促成脊柱转移瘤持久影像学控制的因素,以阐明成功治疗的指征和剂量要求。方法:评估在单一机构接受脊柱立体定向放射治疗(SRS)作为一线治疗的所有患者治疗部位的局部进展情况,局部进展定义为治疗肿瘤的影像学增大和/或活检证实有活跃肿瘤细胞。所有患者每3 - 6个月进行CT、PET或MRI检查直至死亡。治疗决策由放射肿瘤学家、神经外科医生和神经放射学家组成的多学科团队做出。根据国际共识指南定义靶区体积,并在多学科会议上进行审查。每例均采用图像引导技术和调强放疗。分析肿瘤的组织学类型、大体肿瘤体积(GTV)、覆盖GTV 95%的剂量(GTV D95)、处方剂量的95%所覆盖的GTV百分比(GTV V95)、计划靶区体积(PTV)覆盖PTV 95%的剂量(PTV D95)以及处方剂量的95%所覆盖的PTV百分比(PTV V95)与局部控制的相关性,并根据局部进展时间分析其显著性。结果:2003年至2015年期间,单一机构共657例患者接受了811个病灶的治疗。整个队列的平均随访时间和总生存期为26.9个月(范围2 - 141个月)。共有28个病灶进展,平均失败时间为26个月(范围9.7 - 57个月)。中位处方剂量为2400 cGy(范围1600 - 2600 cGy)。在单因素分析中,GTV D95和PTV D95均与局部失败高度显著相关,但GTV、PTV和组织学类型未达到统计学显著性。队列中GTV D95等于或高于1830 cGy切点(高剂量)的患者,其GTV D95中位数为2356 cGy,而接受低于1830 cGy(低剂量)的患者队列中,该值为1709 cGy。就PTV D95而言,等于或高于1740 cGy切点(高剂量)的病灶,其PTV D95中位数为2233 cGy,而低于PTV D95 1740 cGy切点(低剂量)的病灶,该值为1644 cGy。结论:高剂量单次SRS可提供持久的长期控制,无论组织学结果或肿瘤大小如何。在本分析中,预测局部控制的唯一显著因素与实际给予的放射剂量有关。尽管靶区体积用预期剂量得到了良好治疗,但接受较高剂量照射的病灶(中位GTV D95 2356 cGy,最低1830 cGy)比接受较低剂量照射的病灶(中位PTV D95 2232 cGy,最低1740 cGy)具有显著更高的持久局部控制概率(p < 0.001)。高剂量队列患者的局部失败累积率为2%。组织学结果与局部失败无关,这表明放射抗拒的组织学类型尤其从放射外科治疗中获益。对于预后良好的患者,较高剂量的SRS对长期预后很重要。