Ssewanyana Isaac, Arinaitwe Emmanuel, Nankabirwa Joaniter I, Yeka Adoke, Sullivan Richard, Kamya Moses R, Rosenthal Philip J, Dorsey Grant, Mayanja-Kizza Harriet, Drakeley Chris, Greenhouse Bryan, Tetteh Kevin K A
Infectious Diseases Research Collaboration, Kampala, Uganda.
London School of Hygiene and Tropical Medicine, London, UK.
Malar J. 2017 Feb 10;16(1):67. doi: 10.1186/s12936-017-1721-3.
People living in malaria endemic areas acquire protection from severe malaria quickly, but protection from clinical disease and control of parasitaemia is acquired only after many years of repeated infections. Antibodies play a central role in protection from clinical disease; however, protective antibodies are slow to develop. This study sought to investigate the influence of Plasmodium falciparum exposure on the acquisition of high-avidity antibodies to P. falciparum antigens, which may be associated with protection.
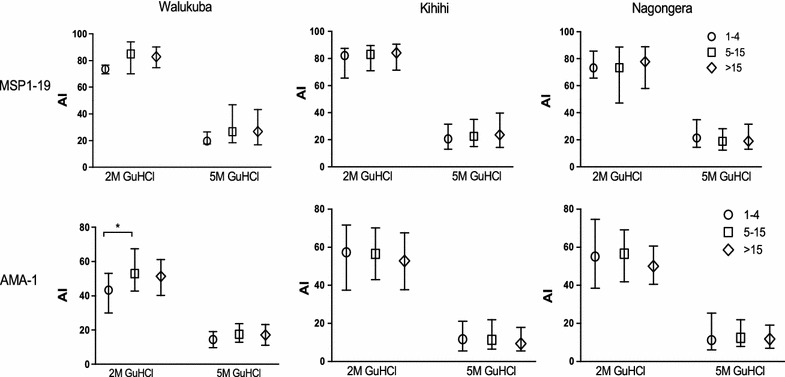
Cross-sectional surveys were performed in children and adults at three sites in Uganda with varied P. falciparum transmission intensity (entomological inoculation rates; 3.8, 26.6, and 125 infectious bites per person per year). Sandwich ELISA was used to measure antibody responses to two P. falciparum merozoite surface antigens: merozoite surface protein 1-19 (MSP1-19) and apical membrane antigen 1 (AMA1). In individuals with detectable antibody levels, guanidine hydrochloride (GuHCl) was added to measure the relative avidity of antibody responses by ELISA.
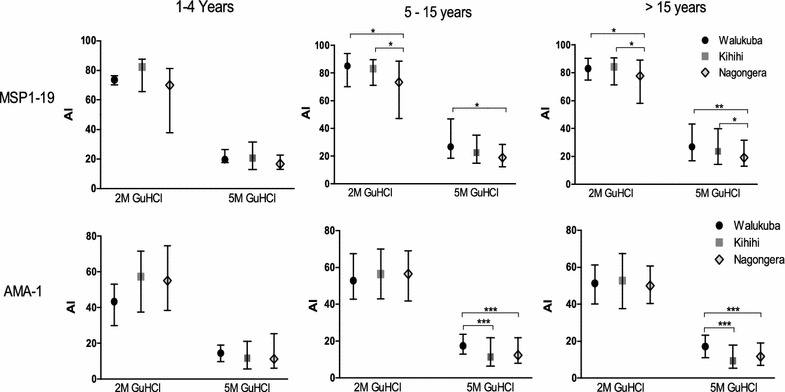
Within a site, there were no significant differences in median antibody levels between the three age groups. Between sites, median antibody levels were generally higher in the higher transmission sites, with differences more apparent for AMA-1 and in ≥5 year group. Similarly, median avidity index (proportion of high avidity antibodies) showed no significant increase with increasing age but was significantly lower at sites of higher transmission amongst participants ≥5 years of age. Using 5 M GuHCl, the median avidity indices in the ≥5 year group at the highest and lowest transmission sites were 19.9 and 26.8, respectively (p = 0.0002) for MSP1-19 and 12.2 and 17.2 (p = 0.0007) for AMA1.
Avidity to two different P. falciparum antigens was lower in areas of high transmission intensity compared to areas with lower transmission. Appreciation of the mechanisms behind these findings as well as their clinical consequences will require additional investigation, ideally utilizing longitudinal data and investigation of a broader array of responses.
生活在疟疾流行地区的人们能迅速获得针对重症疟疾的保护,但只有在多年反复感染后才能获得针对临床疾病的保护以及对寄生虫血症的控制。抗体在预防临床疾病方面发挥着核心作用;然而,保护性抗体的产生较为缓慢。本研究旨在调查恶性疟原虫暴露对获得针对恶性疟原虫抗原的高亲和力抗体的影响,这种抗体可能与保护作用相关。
在乌干达三个恶性疟原虫传播强度不同(昆虫接种率;每人每年3.8、26.6和125次感染性叮咬)的地点,对儿童和成人进行横断面调查。采用夹心ELISA法检测对两种恶性疟原虫裂殖子表面抗原的抗体反应:裂殖子表面蛋白1-19(MSP1-19)和顶端膜抗原1(AMA1)。在抗体水平可检测的个体中,加入盐酸胍(GuHCl)通过ELISA法测量抗体反应的相对亲和力。
在一个地点内,三个年龄组的抗体水平中位数无显著差异。在不同地点之间,传播率较高的地点抗体水平中位数总体较高,AMA-1以及≥5岁组的差异更为明显。同样,中位亲和力指数(高亲和力抗体的比例)并未随年龄增长而显著增加,但在≥5岁参与者中,传播率较高的地点该指数显著较低。使用5M GuHCl,在最高和最低传播地点的≥5岁组中,MSP1-19的中位亲和力指数分别为19.9和26.8(p = 0.0002),AMA1的分别为12.2和17.2(p = 0.0007)。
与传播强度较低的地区相比,在传播强度较高的地区,对两种不同恶性疟原虫抗原的亲和力较低。要了解这些发现背后的机制及其临床后果,还需要进一步研究,理想情况下利用纵向数据并对更广泛的反应进行调查。