Young Lawrence H, Viscoli Catherine M, Curtis Jeptha P, Inzucchi Silvio E, Schwartz Gregory G, Lovejoy Anne M, Furie Karen L, Gorman Mark J, Conwit Robin, Abbott J Dawn, Jacoby Daniel L, Kolansky Daniel M, Pfau Steven E, Ling Frederick S, Kernan Walter N
From Yale University School of Medicine, New Haven, CT (L.H.Y., C.M.V., J.P.C., S.E.I., A.M.L., D.L.J., S.E.P., W.N.K.); Denver VA Medical Center and University of Colorado School of Medicine (G.G.S., J.D.A.); Alpert Medical School of Brown University, Providence, RI (K.L.F., J.D.A.); Maine Medical Center, Portland (M.J.G.); National Institutes of Health/National Institute of Neurological Disorders and Stroke, Bethesda, MD (R.C.); University of Pennsylvania Perelman School of Medicine, Philadelphia (D.M.K.); and University of Rochester School of Medicine and Dentistry, NY (F.S.L.).
Circulation. 2017 May 16;135(20):1882-1893. doi: 10.1161/CIRCULATIONAHA.116.024863. Epub 2017 Feb 28.
Insulin resistance is highly prevalent among patients with atherosclerosis and is associated with an increased risk for myocardial infarction (MI) and stroke. The IRIS trial (Insulin Resistance Intervention after Stroke) demonstrated that pioglitazone decreased the composite risk for fatal or nonfatal stroke and MI in patients with insulin resistance without diabetes mellitus, after a recent ischemic stroke or transient ischemic attack. The type and severity of cardiac events in this population and the impact of pioglitazone on these events have not been described.
We performed a secondary analysis of the effects of pioglitazone, in comparison with placebo, on acute coronary syndromes (MI and unstable angina) among IRIS participants. All potential acute coronary syndrome episodes were adjudicated in a blinded fashion by an independent clinical events committee.
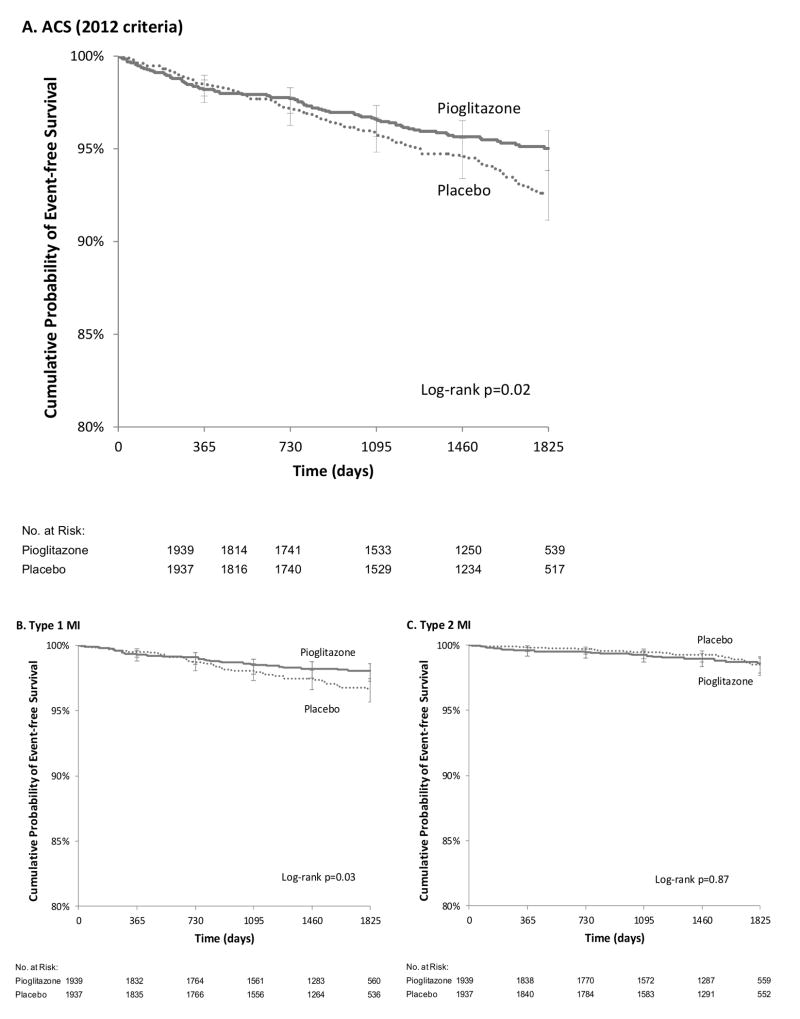
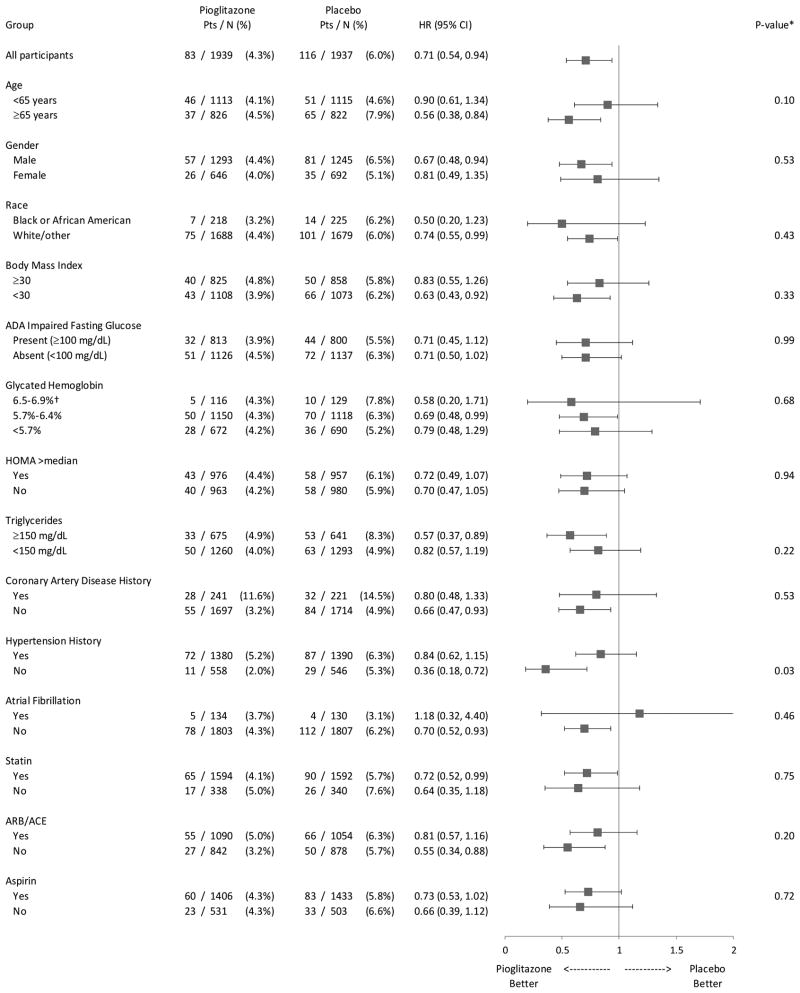
The study cohort was composed of 3876 IRIS participants, mean age 63 years, 65% male, 89% white race, and 12% with a history of coronary artery disease. Over a median follow-up of 4.8 years, there were 225 acute coronary syndrome events, including 141 MIs and 84 episodes of unstable angina. The MIs included 28 (19%) with ST-segment elevation. The majority of MIs were type 1 (94, 65%), followed by type 2 (45, 32%). Serum troponin was 10× to 100× upper limit of normal in 49 (35%) and >100× upper limit of normal in 39 (28%). Pioglitazone reduced the risk of acute coronary syndrome (hazard ratio, 0.71; 95% confidence interval, 0.54-0.94; =0.02). Pioglitazone also reduced the risk of type 1 MI (hazard ratio, 0.62; 95% confidence interval, 0.40-0.96; log-rank =0.03), but not type 2 MI (hazard ratio, 1.05; 95% confidence interval, 0.58-1.91; =0.87). Similarly, pioglitazone reduced the risk of large MIs with serum troponin >100× upper limit of normal (hazard ratio, 0.44; 95% confidence interval, 0.22-0.87; =0.02), but not smaller MIs.
Among patients with insulin resistance without diabetes mellitus, pioglitazone reduced the risk for acute coronary syndromes after a recent cerebrovascular event. Pioglitazone appeared to have its most prominent effect in preventing spontaneous type 1 MIs.
URL: http://clinicaltrials.gov. Unique identifier: NCT00091949.
胰岛素抵抗在动脉粥样硬化患者中非常普遍,并且与心肌梗死(MI)和中风风险增加相关。IRIS试验(中风后胰岛素抵抗干预试验)表明,对于近期发生缺血性中风或短暂性脑缺血发作且无糖尿病的胰岛素抵抗患者,吡格列酮可降低致命或非致命性中风和MI的综合风险。该人群中心脏事件的类型和严重程度以及吡格列酮对这些事件的影响尚未见描述。
我们对IRIS参与者中吡格列酮与安慰剂相比对急性冠状动脉综合征(MI和不稳定型心绞痛)的影响进行了二次分析。所有潜在的急性冠状动脉综合征发作均由独立的临床事件委员会以盲法判定。
研究队列由3876名IRIS参与者组成,平均年龄63岁,65%为男性,89%为白种人,12%有冠状动脉疾病史。在中位随访4.8年期间,有225例急性冠状动脉综合征事件,包括141例MI和84例不稳定型心绞痛发作。MI包括28例(19%)ST段抬高型。大多数MI为1型(94例,65%),其次是2型(45例,32%)。49例(35%)患者血清肌钙蛋白为正常上限的10倍至100倍,39例(28%)患者血清肌钙蛋白>正常上限的100倍。吡格列酮降低了急性冠状动脉综合征的风险(风险比,0.71;95%置信区间,0.54 - 0.94;P = 0.02)。吡格列酮还降低了1型MI的风险(风险比,0.62;95%置信区间,0.40 - 0.96;对数秩检验P = 0.03),但未降低2型MI的风险(风险比,1.05;95%置信区间,0.58 - 1.91;P = 0.87)。同样,吡格列酮降低了血清肌钙蛋白>正常上限100倍的大面积MI的风险(风险比,0.44;95%置信区间,0.22 - 0.87;P = 0.02),但未降低小面积MI的风险。
在近期发生脑血管事件且无糖尿病的胰岛素抵抗患者中,吡格列酮降低了急性冠状动脉综合征的风险。吡格列酮在预防自发性1型MI方面似乎具有最显著的效果。