Armstrong Paul C, Hoefer Thomas, Knowles Rebecca B, Tucker Arthur T, Hayman Melissa A, Ferreira Plinio M, Chan Melissa V, Warner Timothy D
From The William Harvey Research Institute, Barts & the London School of Medicine & Dentistry, Queen Mary University of London, Charterhouse Square, London, United Kingdom.
Arterioscler Thromb Vasc Biol. 2017 May;37(5):949-956. doi: 10.1161/ATVBAHA.116.308763. Epub 2017 Mar 9.
Aspirin together with thienopyridine P2Y inhibitors, commonly clopidogrel, is a cornerstone of antiplatelet therapy. However, many patients receiving this therapy display high on-treatment platelet reactivity, which is a major therapeutic hurdle to the prevention of recurrent thrombotic events. The emergence of uninhibited platelets after thrombopoiesis has been proposed as a contributing factor to high on-treatment platelet reactivity. Here, we investigate the influences of platelet turnover on platelet aggregation in the face of different dual-antiplatelet therapy strategies.
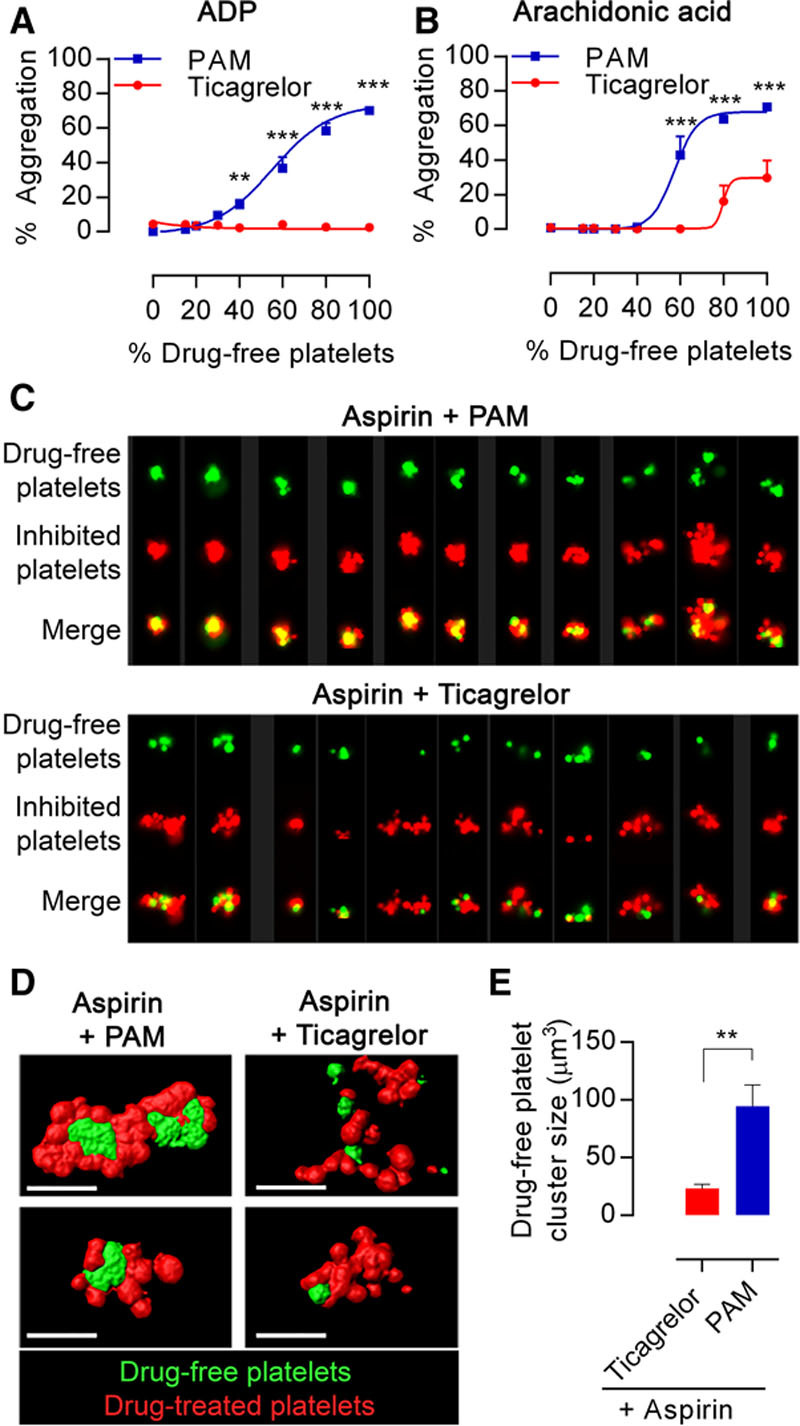
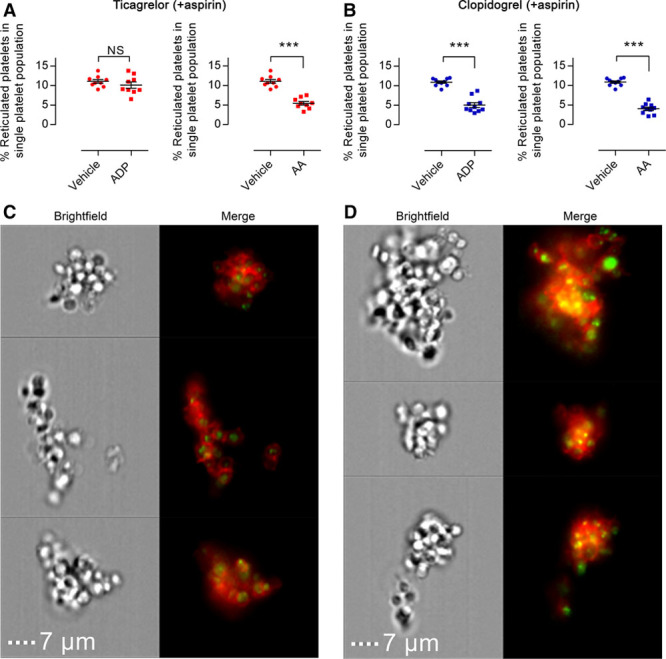
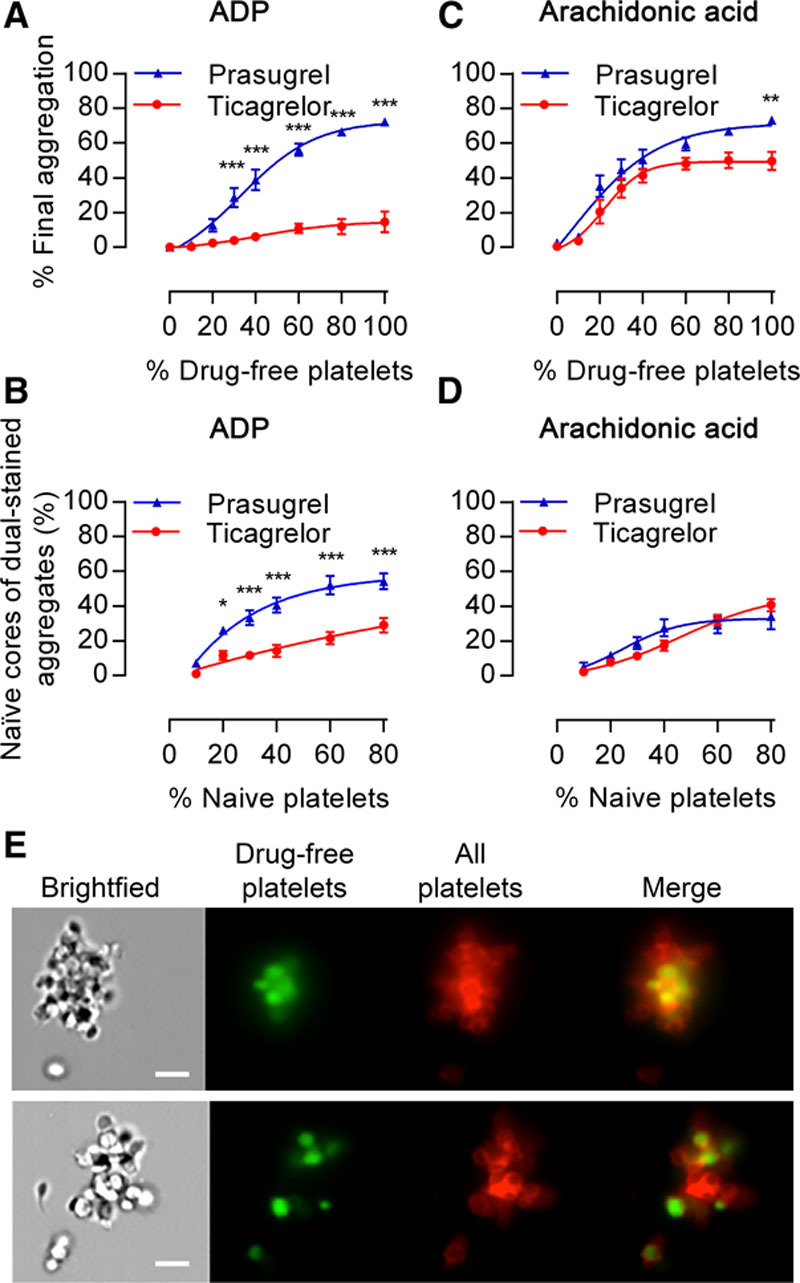
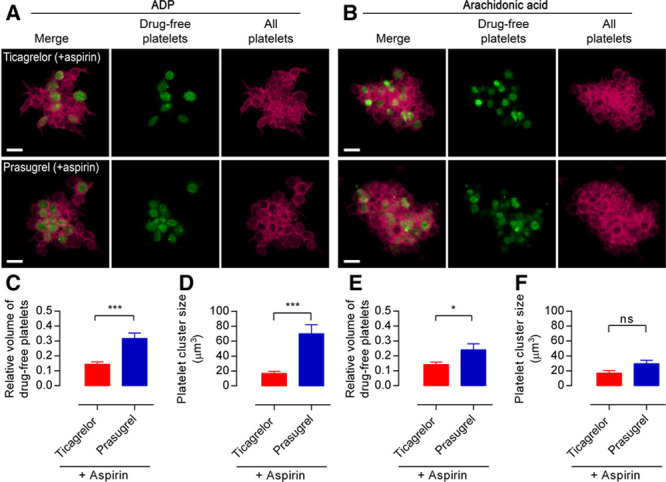
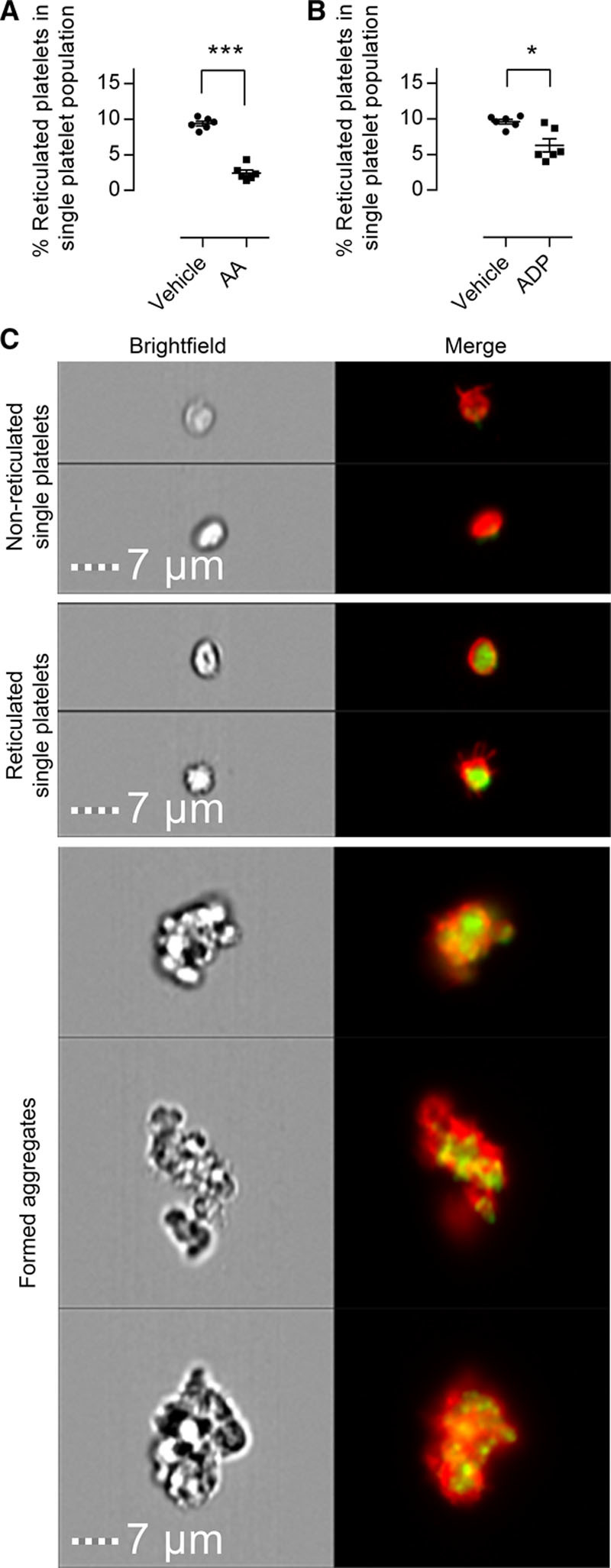
Traditional light transmission aggregometry, cytometry, advanced flow cytometric imaging, and confocal microscopy were used to follow the interactions of populations of platelets from healthy volunteers and patients with stable cardiovascular disease. Newly formed, reticulated platelets overproportionately contributed to, and clustered at, the core of forming aggregates. This phenomenon was particularly observed in samples from patients treated with aspirin plus a thienopyridine, but was absent in samples taken from patients treated with aspirin plus ticagrelor.
Reticulated platelets are more reactive than older platelets and act as seeds for the formation of platelet aggregates even in the presence of antiplatelet therapy. This is coherent with the emergence of an uninhibited subpopulation of reticulated platelets during treatment with aspirin plus thienopyridine, explained by the short pharmacokinetic half-lives of these drugs. This phenomenon is absent during treatment with ticagrelor, because of its longer half-life and ability to act as a circulating inhibitor. These data highlight the important influences of pharmacokinetics on antiplatelet drug efficacies, especially in diseases associated with increased platelet turnover.
阿司匹林与噻吩吡啶类P2Y抑制剂(通常为氯吡格雷)联合使用是抗血小板治疗的基石。然而,许多接受这种治疗的患者表现出较高的治疗期间血小板反应性,这是预防复发性血栓事件的主要治疗障碍。血小板生成后未受抑制的血小板的出现被认为是治疗期间血小板反应性高的一个促成因素。在此,我们研究面对不同的双联抗血小板治疗策略时血小板更新对血小板聚集的影响。
使用传统的光透射聚集测定法、细胞计数法、先进的流式细胞成像法和共聚焦显微镜来追踪健康志愿者和稳定心血管疾病患者的血小板群体之间的相互作用。新形成的网织血小板在形成的聚集体核心中过度贡献并聚集。这种现象在接受阿司匹林加噻吩吡啶治疗的患者样本中尤为明显,但在接受阿司匹林加替格瑞洛治疗的患者样本中未观察到。
网织血小板比衰老血小板更具反应性,即使在存在抗血小板治疗的情况下也可作为血小板聚集体形成的种子。这与阿司匹林加噻吩吡啶治疗期间出现未受抑制的网织血小板亚群相一致,这可以用这些药物较短的药代动力学半衰期来解释。在替格瑞洛治疗期间不存在这种现象,因为其半衰期较长且能够作为循环抑制剂发挥作用。这些数据突出了药代动力学对抗血小板药物疗效的重要影响,尤其是在与血小板更新增加相关的疾病中。