Raoof Mustafa, Dumitra Sinziana, Ituarte Philip H G, Melstrom Laleh, Warner Susanne G, Fong Yuman, Singh Gagandeep
Department of Surgery, City of Hope National Medical Center, Duarte, California.
JAMA Surg. 2017 May 17;152(5):e170117. doi: 10.1001/jamasurg.2017.0117.
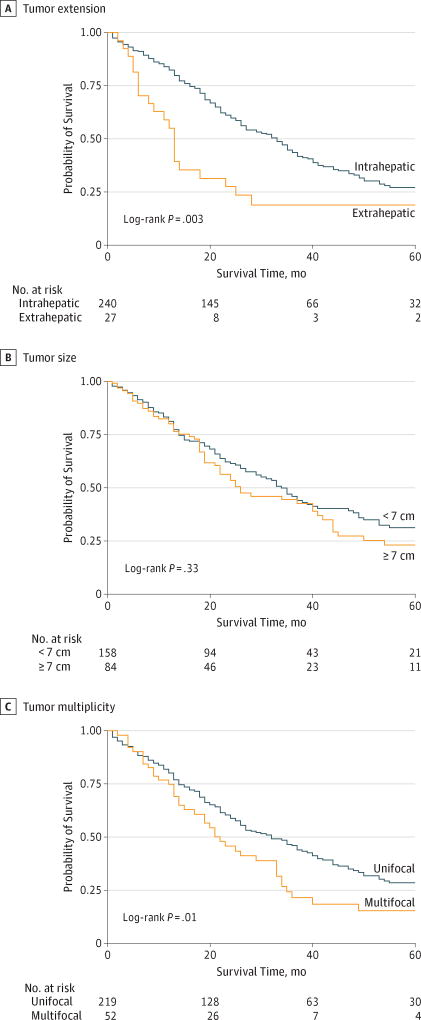
In patients with intrahepatic cholangiocarcinoma (ICC), the oncologic benefit of surgery and perioperative outcomes for large multifocal tumors or tumors with contiguous organ involvement remain to be defined.
To develop and externally validate a simplified prognostic score for ICC and to determine perioperative outcomes for large multifocal ICCs or tumors with contiguous organ involvement.
DESIGN, SETTING, AND PARTICIPANTS: This study of a contemporary cohort merged data from the California Cancer Registry (January 1, 2004, through December 31, 2011) and the Office of Statewide Health Planning and Development inpatient database. Clinicopathologic variables were compared between tumors that were intrahepatic, small (<7 cm), and solitary (ISS) and those that had extrahepatic extension and were large (≥7 cm) and multifocal (ELM). External validation of the prognostic model was performed using an independent data set from the National Cancer Institute's Surveillance, Epidemiology, and End Results database from January 1, 2004, through December 31, 2013.
Patient overall survival after hepatectomy.
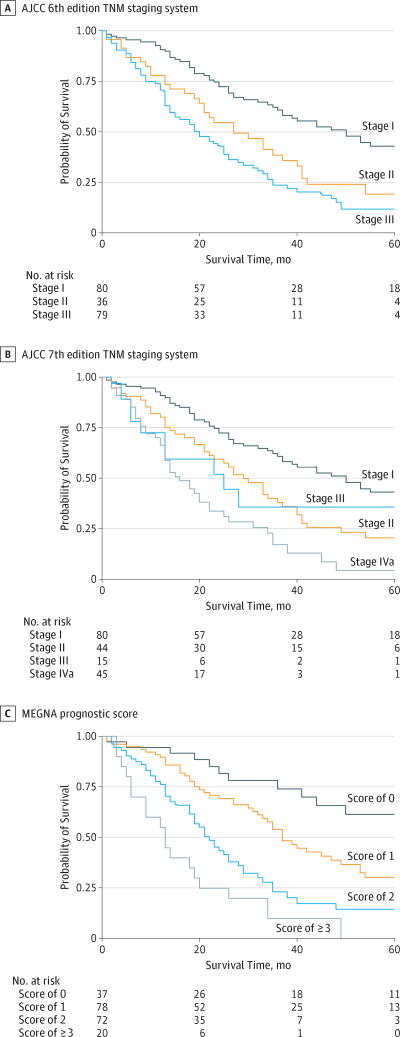
A total of 275 patients (123 men [44.7%] and 152 women [55.3%]; median [interquartile range] age, 65 [55-72] years) met the inclusion criteria. No significant differences in overall complication rate (ISS, 48 [34.5%]; ELM, 37 [27.2%]; P = .19) and mortality rate (ISS, 10 [7.2%]; ELM, 6 [4.4%]; P = .32) were found. A multivariate Cox proportional hazards model demonstrated that multifocality, extrahepatic extension, grade, node positivity, and age greater than 60 years are independently associated with worse overall survival. These variables were used to develop the MEGNA prognostic score. The prognostic separation/discrimination index was improved with the MEGNA prognostic score (0.21; 95% CI, 0.11-0.33) compared with the staging systems of the American Joint Committee on Cancer sixth (0.17; 95% CI, 0.09-0.29) and seventh (0.18; 95% CI, 0.08-0.30) editions.
The MEGNA prognostic score allows more accurate and superior estimation of patient survival after hepatectomy compared with current staging systems.
在肝内胆管癌(ICC)患者中,手术对大的多灶性肿瘤或累及相邻器官的肿瘤的肿瘤学获益及围手术期结局仍有待明确。
开发并外部验证一种简化的ICC预后评分系统,并确定大的多灶性ICC或累及相邻器官的肿瘤的围手术期结局。
设计、设置和参与者:这项针对当代队列的研究合并了加利福尼亚癌症登记处(2004年1月1日至2011年12月31日)和全州卫生规划与发展办公室住院患者数据库的数据。比较了肝内、小(<7 cm)且孤立(ISS)的肿瘤与有肝外扩展、大(≥7 cm)且多灶(ELM)的肿瘤之间的临床病理变量。使用来自美国国立癌症研究所监测、流行病学和最终结果数据库(2004年1月1日至2013年12月31日)的独立数据集对预后模型进行外部验证。
肝切除术后患者的总生存期。
共有275例患者(123例男性[44.7%]和152例女性[55.3%];中位[四分位间距]年龄,65[55 - 72]岁)符合纳入标准。总体并发症发生率(ISS组,48例[34.5%];ELM组,37例[27.2%];P = 0.19)和死亡率(ISS组,10例[7.2%];ELM组,6例[4.4%];P = 0.32)无显著差异。多变量Cox比例风险模型表明,多灶性、肝外扩展、分级、淋巴结阳性以及年龄大于60岁与较差的总生存期独立相关。这些变量被用于开发MEGNA预后评分系统。与美国癌症联合委员会第六版(0.17;95%CI,0.09 - 0.29)和第七版(0.18;95%CI,0.08 - 0.30)分期系统相比,MEGNA预后评分系统的预后区分/鉴别指数有所提高(0.21;95%CI,0.11 - 0.33)。
与当前分期系统相比,MEGNA预后评分系统能够更准确、更优地估计肝切除术后患者的生存期。