Brondani Rosane, Garcia de Almeida Andrea, Abrahim Cherubini Pedro, Mandelli Mota Suelen, de Alencastro Luiz Carlos, Antunes Apio Cláudio Martins, Bianchin Muxfeldt Marino
Postgraduate Program in Medicine: Medical Science, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil.
Basic Research and Advanced Investigations in Neurology (B.R.A.I.N.), Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil.
Cerebrovasc Dis Extra. 2017;7(1):51-61. doi: 10.1159/000458730. Epub 2017 Mar 30.
Decompressive hemicraniectomy (DHC) is a life-saving procedure for treatment of large malignant middle cerebral artery (MCA) strokes. Post-stroke epilepsy is an additional burden for these patients, but its incidence and the risk factors for its development have been poorly investigated.
To report the prevalence and risk factors for post-stroke seizures and post-stroke epilepsy after DHC for treatment of large malignant MCA strokes in a cohort of 36 patients.
In a retrospective cohort study of 36 patients we report the timing and incidence of post-stroke epilepsy. We analyzed if age, sex, vascular risk factors, side of ischemia, reperfusion therapy, stroke etiology, extension of stroke, hemorrhagic transformation, ECASS scores, National Institutes of Health Stroke Scale (NIHSS) scores, or modified Rankin scores were risk factors for seizure or epilepsy after DHC for treatment of large MCA strokes.
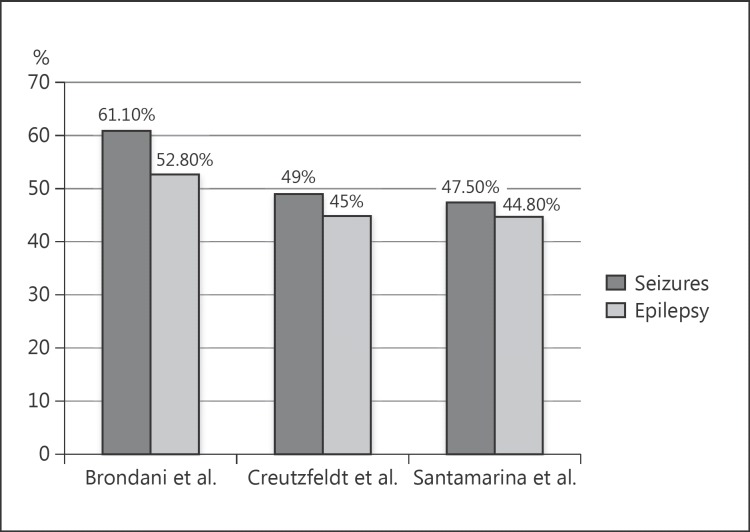
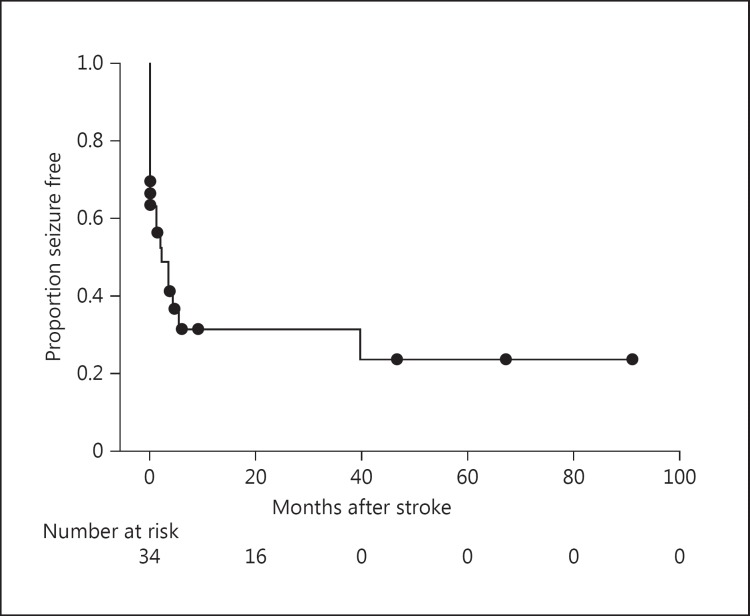
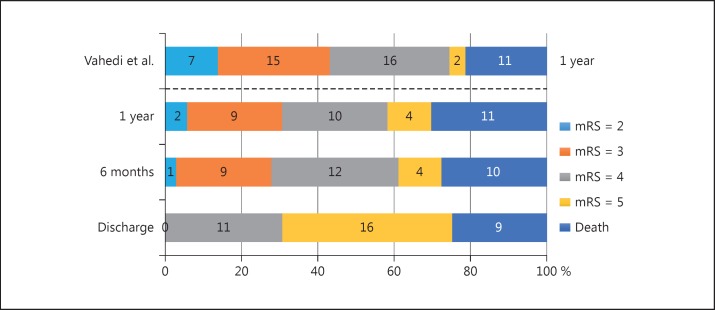
The mean patient follow-up time was 1,086 days (SD = 1,172). Out of 36 patients, 9 (25.0%) died before being discharged. After 1 year, a total of 11 patients (30.6%) had died, but 22 (61.1%) of them had a modified Rankin score ≤4. Thirteen patients (36.1%) developed seizures within the first week after stroke. Seizures occurred in 22 (61.1%) of 36 patients (95% CI = 45.17-77.03%). Out of 34 patients who survived the acute period, 19 (55.9%) developed epilepsy after MCA infarcts and DHC (95% CI = 39.21-72.59%). In this study, no significant differences were observed between the patients who developed seizures or epilepsy and those who remained free of seizures or epilepsy regarding age, sex, side of stroke, presence of the clinical risk factors studied, hemorrhagic transformation, time of craniectomy, and Rankin score after 1 year of stroke.
CONCLUSION: The incidence of seizures and epilepsy after malignant MCA infarcts submitted to DHC might be very high. Seizure might occur precociously in patients who are not submitted to anticonvulsant prophylaxis. The large stroke volume and the large cortical ischemic area seem to be the main risk factors for seizure or epilepsy development in this subtype of stroke. .
减压性去骨瓣开颅术(DHC)是治疗大面积恶性大脑中动脉(MCA)卒中的一种挽救生命的手术。卒中后癫痫是这些患者的额外负担,但其发病率及其发生的危险因素尚未得到充分研究。
报告36例接受DHC治疗大面积恶性MCA卒中患者的卒中后癫痫发作和卒中后癫痫的患病率及危险因素。
在一项对36例患者的回顾性队列研究中,我们报告了卒中后癫痫的发生时间和发病率。我们分析了年龄、性别、血管危险因素、缺血侧、再灌注治疗、卒中病因、卒中范围、出血转化、欧洲急性卒中协作研究(ECASS)评分、美国国立卫生研究院卒中量表(NIHSS)评分或改良Rankin评分是否为接受DHC治疗大面积MCA卒中后癫痫发作或癫痫的危险因素。
患者的平均随访时间为1086天(标准差=1172)。36例患者中,9例(25.0%)在出院前死亡。1年后,共有11例患者(30.6%)死亡,但其中22例(61.1%)的改良Rankin评分为≤4分。13例患者(36.1%)在卒中后的第一周内发生癫痫发作。36例患者中有22例(61.1%)发生癫痫发作(95%可信区间=45.17-77.03%)。在急性期存活的34例患者中,19例(55.9%)在MCA梗死和DHC后发生癫痫(95%可信区间=39.21-72.59%)。在本研究中,在发生癫痫发作或癫痫的患者与未发生癫痫发作或癫痫的患者之间,在年龄、性别、卒中侧、所研究的临床危险因素的存在情况、出血转化、颅骨切除术时间和卒中1年后的Rankin评分方面未观察到显著差异。
接受DHC治疗的恶性MCA梗死患者癫痫发作和癫痫的发生率可能非常高。未接受抗惊厥预防的患者可能较早发生癫痫发作。大面积卒中体积和大面积皮质缺血区域似乎是该亚型卒中癫痫发作或癫痫发生的主要危险因素。