Zane Nicole R, Reedy Michael D, Gastonguay Marc R, Himebauch Adam S, Ramsey Evan Z, Topjian Alexis A, Zuppa Athena F
1Center for Clinical Pharmacology, The Children's Hospital of Philadelphia, Philadelphia, PA. 2Department of Pharmacy, Nemours Alfred I. DuPont Hospital for Children, Wilmington, DE. 3Metrum Research Group, Tariffville, CT. 4Department of Anesthesiology and Critical Care Medicine, The Children's Hospital of Philadelphia, Philadelphia, PA.
Pediatr Crit Care Med. 2017 Jul;18(7):e290-e297. doi: 10.1097/PCC.0000000000001198.
Limited data exist on the effects of therapeutic hypothermia on renal function and pharmacokinetics in pediatric patients after cardiac arrest. The objective was to describe the differences in vancomycin disposition in pediatric patients following cardiac arrest treated with either therapeutic hypothermia or normothermia using population pharmacokinetic modeling.
Single-center, retrospective cohort study.
A tertiary care hospital pediatric and cardiac ICU.
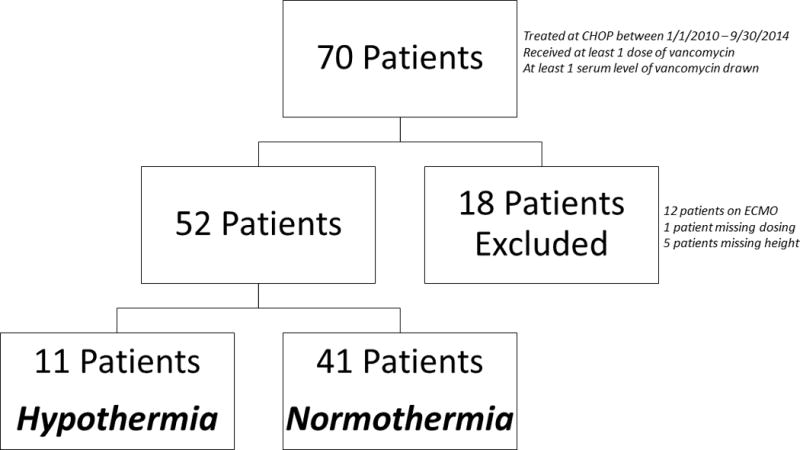
Fifty-two pediatric patients (30 d to 17 yr old) who experienced a cardiac arrest, received vancomycin, and were treated with therapeutic hypothermia (32-34°C) or normothermia (36.3-37.6°C) between January 1, 2010, and September 30, 2014, were reviewed.
None.
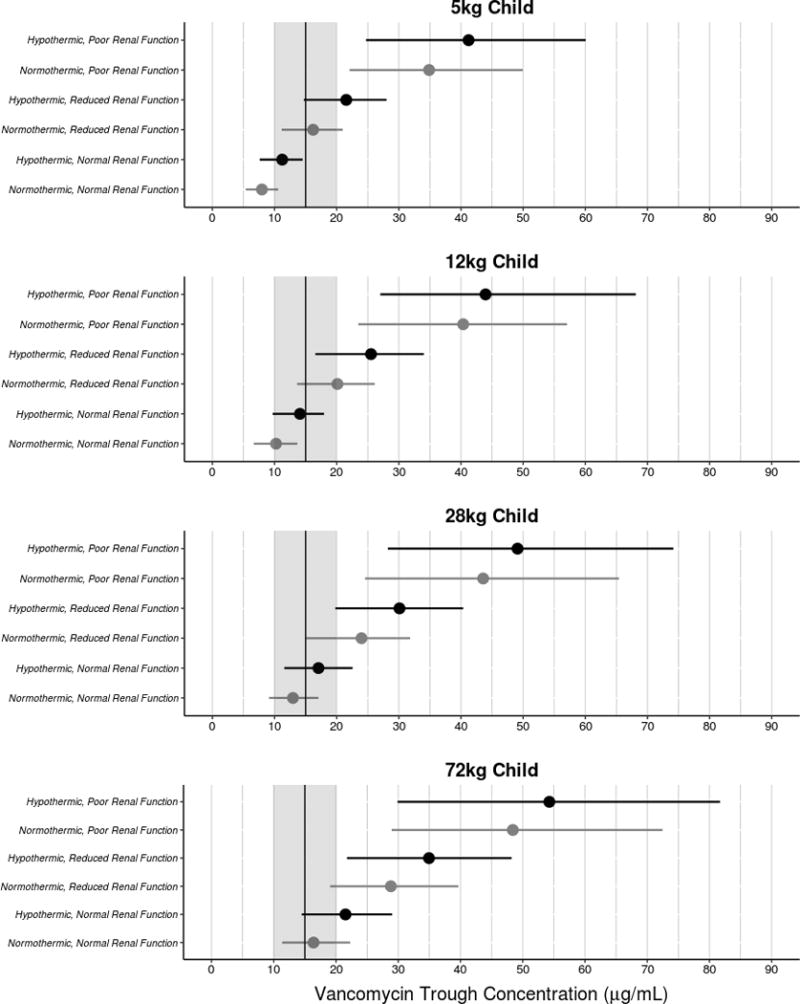
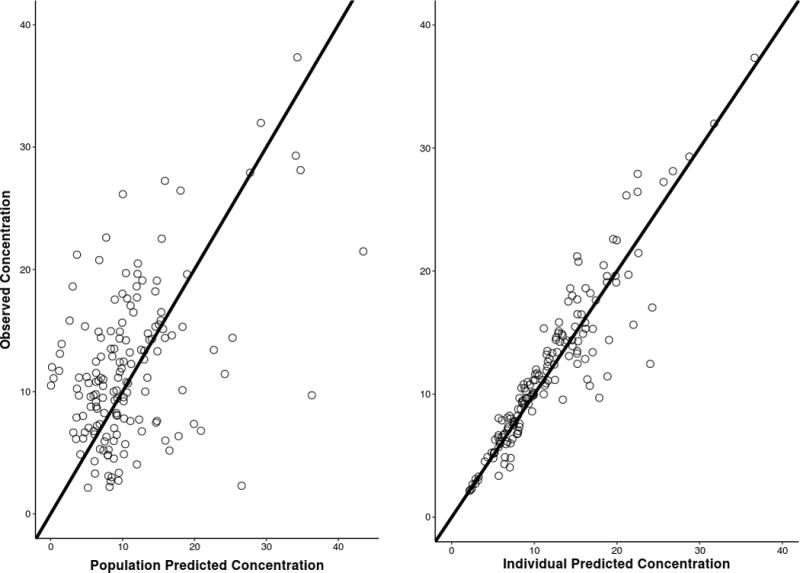
A two-compartment model with linear elimination, weight effects on clearance, intercompartmental clearance (Q), central volume of distribution (V1), and peripheral volume of distribution (V2) adequately described the data despite high variability due to the small sample size. The typical value of clearance in this study was 4.48 L/hr (0.19 L/hr/kg) for a normothermic patient weighing 70 kg and a glomerular filtration rate of 90 mL/min/1.73 m. Patients treated with normothermia but with reduced or poor renal function (≤ 90 mL/min/1.73 m) had up to an 80% reduction in vancomycin clearance compared to those with normal renal function (90-140 mL/min/1.73 m). Patients with normal renal function but treated with therapeutic hypothermia versus normothermia experienced up to 25% reduction in vancomycin clearance. Patients treated with therapeutic hypothermia and with poor renal function experienced up to an 84% reduction in vancomycin clearance.
Patients receiving hypothermia and/or with decreased renal function had lower vancomycin clearances based on a retrospectively fitted two-compartment model in children who experience cardiac arrest.
关于治疗性低温对心脏骤停后儿科患者肾功能和药代动力学影响的数据有限。本研究目的是通过群体药代动力学建模,描述心脏骤停后接受治疗性低温或常温治疗的儿科患者万古霉素处置的差异。
单中心回顾性队列研究。
一家三级护理医院的儿科和心脏重症监护病房。
回顾了2010年1月1日至2014年9月30日期间经历心脏骤停、接受万古霉素治疗并接受治疗性低温(32 - 34°C)或常温(36.3 - 37.6°C)治疗的52例儿科患者(30天至17岁)。
无。
尽管由于样本量小导致变异性高,但具有线性消除、体重对清除率的影响、隔室间清除率(Q)、中央分布容积(V1)和外周分布容积(V2)的二室模型充分描述了数据。本研究中,对于体重70 kg且肾小球滤过率为90 mL/min/1.73 m²的常温患者,清除率的典型值为4.48 L/hr(0.19 L/hr/kg)。与肾功能正常(90 - 140 mL/min/1.73 m²)的患者相比,肾功能降低或较差(≤ 90 mL/min/1.73 m²)的常温治疗患者万古霉素清除率降低高达80%。肾功能正常但接受治疗性低温而非常温治疗的患者万古霉素清除率降低高达25%。接受治疗性低温且肾功能较差的患者万古霉素清除率降低高达84%。
基于对经历心脏骤停儿童的回顾性拟合二室模型,接受低温治疗和/或肾功能降低的患者万古霉素清除率较低。