Tang Ying, Chen Junzhe, Huang Kai, Luo Dan, Liang Peifen, Feng Min, Chai Wenxin, Fung Erik, Lan Hui Yao, Xu Anping
Department of Nephrology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, 107 Yan Jiang West Road, Guangzhou, China.
Department of Nephrology, The People's Hospital of Meishan City, Meishan, China.
BMC Nephrol. 2017 May 31;18(1):184. doi: 10.1186/s12882-017-0594-6.
Acute kidney injury (AKI) is a severe complication associated with abdominal aortic aneurysm (AAA) repair. In this study, we evaluated the incidence, risk factors and in-hospital mortality of AKI in patients after the AAA repair surgery.
A total of 314 Chinese AAA patients who underwent endovascular aneurysm repair (EVAR) or open aneurysm repair (OPEN) were enrolled in this study. AKI was diagnosed according to the 2012 KDIGO criteria. Logistic regression modeling was used to explore risk factors of AKI, while risk factors associated with in-hospital mortality in AKI patients were investigated using Cox proportional hazards model and Kaplan-Meier analysis, respectively. Multicollinearity analysis was performed to identify the collinearity between the variables before logistic regression analysis and Cox proportional hazards analysis.
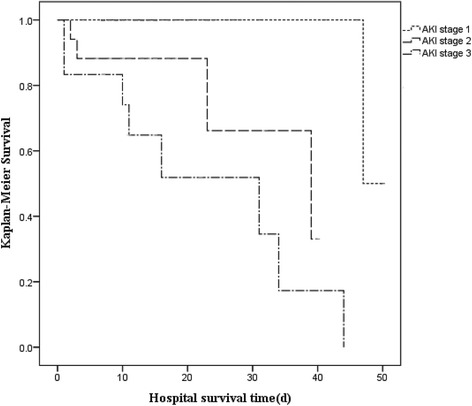
Among 314 patients, 94 (29.9%) developed AKI after AAA repair surgery. Severity of AKI and ruptured AAA were independently associated with an increase in in-hospital mortality in AKI patients after AAA repair. Kaplan-Meier analysis identified severity of AKI as being negatively associated with hospital survival in AKI patients. Risk factors associated with AKI included cardiovascular disease (OR 3.169, 95% confidence interval (CI) 1.538 to 6.527, P = 0.002), decreased eGFR (OR 0.965, 95%CI 0.954 to 0.977, P < 0.001), ruptured AAA (OR 2.717, 95%CI 1.320 to 5.592, P = 0.007), renal artery involvement (OR 2.903, 95%CI 1.219 to 6.912, P = 0.016) and OPEN (OR 2.094, 95%CI 1.048 to 4.183, P = 0.036). Further subgroup analysis identified OPEN as an important risk factor of AKI in ruptured AAA patients but not in ruptured AAA patients. The incidence of AKI was significantly lower in EVAR than in OPEN (27.1% vs. 42.8%) and, similarly lower in nonruptured AAA than in ruptured AAA (26.2% vs. 48.1%).
One-third of AAA patients developed AKI after repair surgery. Severity of AKI was associated with reduced survival rate in AAA patients who developed postoperative AKI. Decreased preoperative creatinine clearance, cardiovascular disease, ruptured AAA and OPEN were independent risk factors for postoperative AKI in all 314 AAA patients. Although a lower rate of incident AKI was observed in EVAR compared with OPEN, subgroup analysis of ruptured AAA versus nonruptured AAA showed that EVAR was an independent protective factor for AKI only in ruptured AAA patients but not in nonruptured AAA patients.
急性肾损伤(AKI)是腹主动脉瘤(AAA)修复术后的一种严重并发症。在本研究中,我们评估了AAA修复术后患者AKI的发生率、危险因素及住院死亡率。
本研究共纳入314例接受血管腔内动脉瘤修复术(EVAR)或开放性动脉瘤修复术(OPEN)的中国AAA患者。根据2012年KDIGO标准诊断AKI。采用逻辑回归模型探索AKI的危险因素,同时分别使用Cox比例风险模型和Kaplan-Meier分析研究AKI患者住院死亡率的相关危险因素。在进行逻辑回归分析和Cox比例风险分析之前,进行多重共线性分析以识别变量之间的共线性。
314例患者中,94例(29.9%)在AAA修复术后发生AKI。AKI的严重程度和破裂性AAA与AAA修复术后AKI患者住院死亡率的增加独立相关。Kaplan-Meier分析确定AKI的严重程度与AKI患者的住院生存率呈负相关。与AKI相关的危险因素包括心血管疾病(比值比[OR]3.169,95%置信区间[CI]1.538至6.527,P = 0.002)、估算肾小球滤过率(eGFR)降低(OR 0.965,95%CI 0.954至0.977,P < 0.001)、破裂性AAA(OR 2.717,95%CI 1.320至5.592,P = 0.007)、肾动脉受累(OR 2.903,95%CI 1.219至6.912,P = 0.016)和OPEN(OR 2.094,95%CI 1.048至4.183,P = 0.036)。进一步的亚组分析确定OPEN是破裂性AAA患者中AKI的重要危险因素,但在未破裂性AAA患者中不是。EVAR组的AKI发生率显著低于OPEN组(27.1%对42.8%),同样,未破裂性AAA组的AKI发生率低于破裂性AAA组(26.2%对48.1%)。
三分之一的AAA患者在修复术后发生AKI。AKI的严重程度与术后发生AKI的AAA患者生存率降低相关。术前肌酐清除率降低、心血管疾病、破裂性AAA和OPEN是所有314例AAA患者术后AKI的独立危险因素。尽管与OPEN相比,EVAR组的AKI发生率较低,但破裂性AAA与未破裂性AAA的亚组分析表明,EVAR仅在破裂性AAA患者中是AKI的独立保护因素,而在未破裂性AAA患者中不是。