Yoo Yung Ju, Yang Hee Kyung, Hwang Jeong-Min
Department of Ophthalmology, Kangwon National University Hospital, Kangwon National University Graduate School of Medicine, Chuncheon, Korea.
Department of Ophthalmology, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
PLoS One. 2017 Jun 2;12(6):e0178361. doi: 10.1371/journal.pone.0178361. eCollection 2017.
To evaluate the efficacy of digital pupillometry in the diagnosis of anisocoria related to Horner syndrome in adult patients.
Retrospective, observational, case control study.
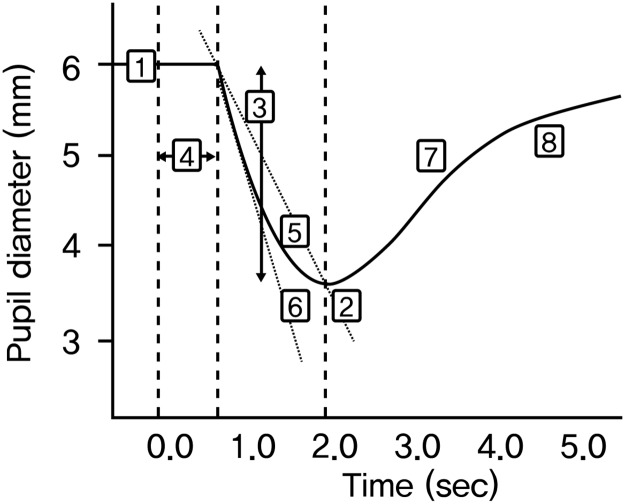
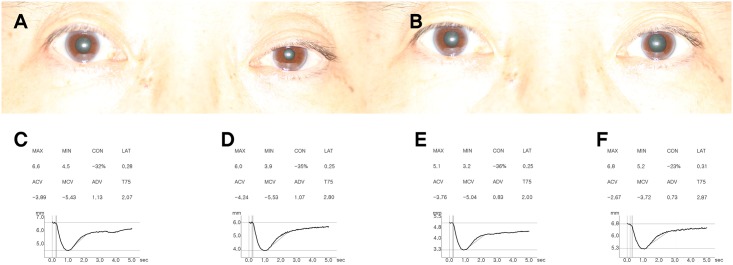
Nineteen patients with unilateral Horner syndrome (Horner group) and age-matched controls of 30 healthy individuals with normal vision and neither optic nerve dysfunction nor pupillary abnormalities were included. Pupillary light reflex (PLR) of the Horner group and controls were measured by a dynamic pupillometer (PLR-200; NeurOptics Inc., Irvine, USA). Minimal and maximal (min/max) pupil diameters, latency, constriction ratio, constriction velocity, dilation velocity, and total time taken by the pupil to recover 75% of maximal pupil diameter (T75) were noted. PLR were measured at baseline in both groups and at 30-45 minutes later after 0.5% apraclonidine (Iopidine®; Alcon Laboratories, Fort Worth, TX, USA) instillation in the Horner group.
The PLR parameters in the affected eye and inter-eye difference before and after 0.5% apraclonidine instillation.
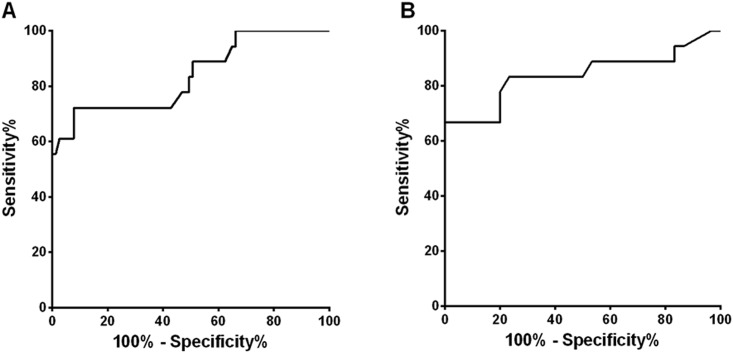
In the Horner group, pupil diameters and T75 showed significant difference between the affected eye and unaffected contralateral eye at baseline (all P<0.00625). Compared to controls, inter-eye difference values of pupil diameters and T75 were significantly larger in the Horner group (all P<0.001). After 0.5% apraclonidine instillation, changes in pupil diameter and constriction ratio were significantly larger in the affected eye compared to the unaffected contralateral eye (all P<0.00625). The area under the receiver operating characteristic curves for diagnosing Horner syndrome were largest for baseline inter-eye difference in min/max pupil sizes (AUC = 0.975, 0.994), T75 (AUC = 0.838), and change in min/max pupil sizes after apraclonidine instillation (AUC = 0.923, 0.929, respectively). The diagnostic criteria for Horner syndrome relying on baseline pupillary measurements was defined as one of the two major findings; 1) smaller maximal pupil diameter in the affected eye with an inter-eye difference of > 0.5 mm, or 2) T75 > 2.61 seconds in the affected eye, which showed a sensitivity of 94.7% and specificity of 93.3%. The diagnostic accuracy of apraclonidine testing showed a sensitivity of 84.6% and specificity of 92.3%.
Digital pupillometry is an objective method for quantifying PLR. Baseline inter-eye difference in maximal pupil sizes and dilation lag measured by T75 was equally effective in the diagnosis of Horner syndrome compared to the reversal of anisocoria after apraclonidine instillation.
评估数字瞳孔测量法在诊断成年患者霍纳综合征相关的瞳孔不等大方面的疗效。
回顾性、观察性病例对照研究。
纳入19例单侧霍纳综合征患者(霍纳组),并选取30名年龄匹配的对照者,这些对照者视力正常,无视神经功能障碍及瞳孔异常。霍纳组和对照组的瞳孔对光反射(PLR)均采用动态瞳孔测量仪(PLR - 200;美国尔湾市NeurOptics公司)进行测量。记录最小和最大(min/max)瞳孔直径、潜伏期、收缩率、收缩速度、扩张速度以及瞳孔恢复至最大瞳孔直径75%所需的总时间(T75)。两组均在基线时测量PLR,霍纳组在滴入0.5%阿可乐定(Iopidine®;美国得克萨斯州沃思堡市爱尔康实验室)后30 - 45分钟再次测量。
0.5%阿可乐定滴入前后患眼及两眼间差异的PLR参数。
在霍纳组中,基线时患眼与对侧未患眼的瞳孔直径和T75存在显著差异(所有P<0.00625)。与对照组相比,霍纳组两眼间瞳孔直径和T75的差异值显著更大(所有P<0.001)。滴入0.5%阿可乐定后,患眼的瞳孔直径和收缩率变化相比对侧未患眼显著更大(所有P<0.00625)。用于诊断霍纳综合征的受试者工作特征曲线下面积,对于基线时两眼间min/max瞳孔大小差异(AUC = 0.975, 0.994)、T75(AUC = 0.838)以及阿可乐定滴入后min/max瞳孔大小变化(AUC分别为0.923, 0.929)最大。基于基线瞳孔测量的霍纳综合征诊断标准被定义为以下两个主要发现之一:1)患眼最大瞳孔直径较小,两眼间差异>0.5 mm,或2)患眼T75>2.61秒,其敏感性为94.7%,特异性为93.3%。阿可乐定试验的诊断准确性显示敏感性为84.6%,特异性为92.3%。
数字瞳孔测量法是一种量化PLR的客观方法。与阿可乐定滴入后瞳孔不等大的逆转相比,通过T75测量的基线时两眼间最大瞳孔大小差异和扩张延迟在诊断霍纳综合征方面同样有效。