Huang Gregory S, Chance Elisha A, Hileman Barbara M, Emerick Eric S, Gianetti Emily A
Trauma and Critical Care Services, St Elizabeth Youngstown Hospital, Youngstown, Ohio, USA.
Department of Sociology, Anthropology, and Gerontology, Youngstown State University, Youngstown, Ohio, USA.
JSLS. 2017 Apr-Jun;21(2). doi: 10.4293/JSLS.2017.00013.
No criteria define indications for laparoscopic splenectomy in trauma. This investigation compared characteristics of trauma patients and outcomes between laparoscopic and open splenectomies.
Patients were identified retrospectively by using ICD-9 codes. Included patients were 18 or older, with a blunt splenic injury from January 1, 2011, through December 31, 2014, and required splenectomy. Excluded patients had penetrating trauma, successful nonoperative management, or successful embolization. Variables included demographics, presenting characteristics, injury severity scores, abdominal abbreviated injury scores, splenic injury grade, surgical indication and approach (open or laparoscopic), surgery length, intra-operative blood loss, transfusions, length of stay, complications, mortality, and discharge disposition.
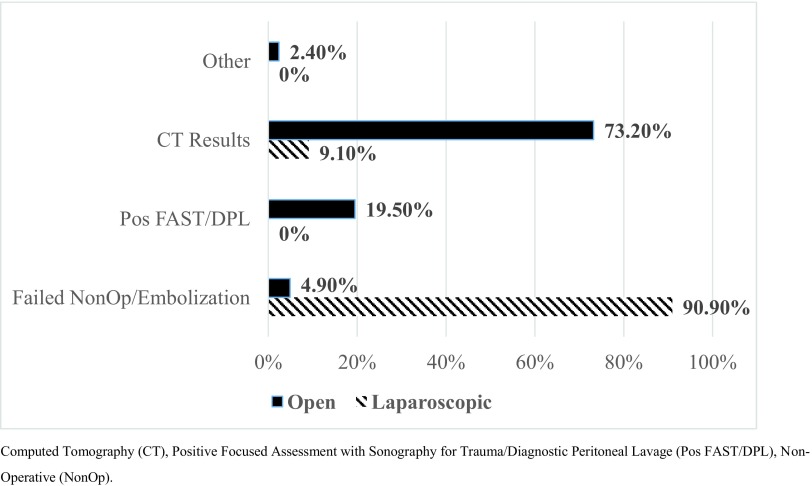
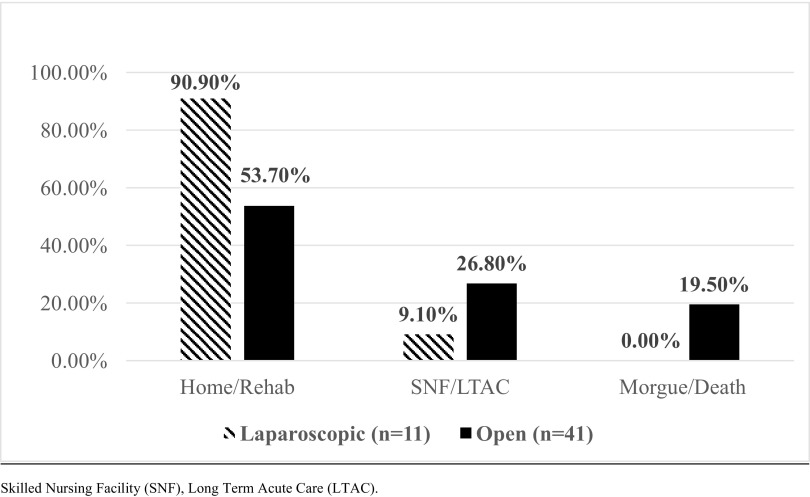
Forty-one patients underwent open splenectomy, and 11 underwent laparoscopic splenectomy. The mean age was 48.7 years, and men comprised the sample majority (36/52). The groups were well matched for age, abdominal injury scores, and admission vital signs. The open group had a significantly lower level of consciousness and more acidosis compared with the laparoscopic group. Most laparoscopic splenectomies were performed after failed nonoperative management or embolization. The indications for open splenectomy were a positive focused assessment with sonography for trauma and computed tomography results. Laparoscopic patients had significantly longer times between presentation and surgery and longer operations, but had significantly less blood loss and fewer transfusions compared with the open group. There were no differences in mortality, length of stay, complications, or discharge dispositions.
Laparoscopic splenectomy is useful in patients with blunt trauma in whom conservative management produced no improvement and who do not have other injuries to preclude laparoscopy.
目前尚无明确标准界定创伤患者行腹腔镜脾切除术的适应证。本研究比较了创伤患者的特征以及腹腔镜脾切除术与开放性脾切除术的治疗效果。
通过国际疾病分类第九版(ICD-9)编码对患者进行回顾性识别。纳入患者年龄在18岁及以上,于2011年1月1日至2014年12月31日期间因钝性脾损伤而需要行脾切除术。排除有穿透性创伤、非手术治疗成功或栓塞成功的患者。变量包括人口统计学资料、临床表现、损伤严重程度评分、腹部简明损伤评分、脾损伤分级、手术适应证及方式(开放或腹腔镜)、手术时长、术中失血量、输血情况、住院时间、并发症、死亡率及出院处置情况。
41例患者接受了开放性脾切除术,11例接受了腹腔镜脾切除术。平均年龄为48.7岁,样本中男性占多数(36/52)。两组在年龄、腹部损伤评分及入院生命体征方面匹配良好。与腹腔镜组相比,开放组患者意识水平明显较低且酸中毒情况更严重。大多数腹腔镜脾切除术是在非手术治疗或栓塞失败后进行的。开放性脾切除术的适应证为创伤超声重点评估阳性及计算机断层扫描结果阳性。与开放组相比,腹腔镜手术患者从就诊到手术的时间及手术时间明显更长,但失血量明显更少且输血次数更少。在死亡率、住院时间、并发症或出院处置方面无差异。
对于钝性创伤患者,若保守治疗无效且无其他损伤妨碍腹腔镜检查,腹腔镜脾切除术是有用的。