Strom Jordan B, Kramer Daniel B, Wang Yun, Shen Changyu, Wasfy Jason H, Landon Bruce E, Wilker Elissa H, Yeh Robert W
Richard A. and Susan F. Smith Center for Cardiovascular Outcomes Research, Division of Cardiovascular Medicine, Beth Israel Deaconess Medical Center, Boston, Massachusetts, United States of America.
Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, Massachusetts, United States of America.
PLoS One. 2017 Jul 10;12(7):e0180767. doi: 10.1371/journal.pone.0180767. eCollection 2017.
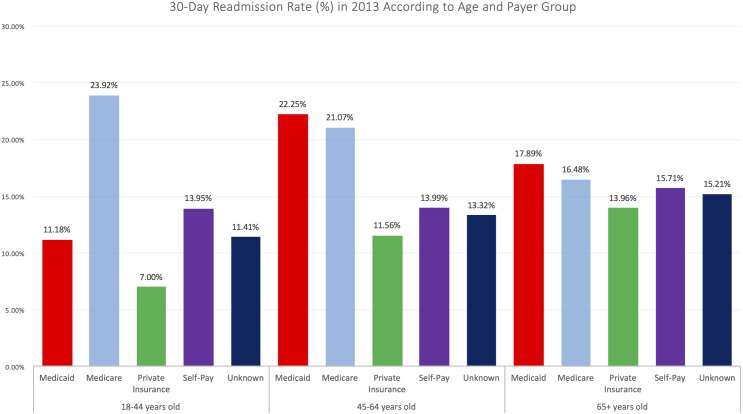
Few studies have examined rates and causes of short-term readmissions among adults across age and insurance types. We compared rates, characteristics, and costs of 30-day readmission after all-cause hospitalizations across insurance types in the US. We retrospectively evaluated alive patients ≥18 years old, discharged for any cause, 1/1/13-11/31/13, 2006 non-federal hospitals in 21 states in the Nationwide Readmissions Database. The primary stratification variable of interest was primary insurance. Comorbid conditions were assessed based on Elixhauser comorbidities, as defined by administrative billing codes. Additional measures included diagnoses for index hospitalizations leading to rehospitalization. Hierarchical multivariable logistic regression models, with hospital site as a random effect, were used to calculate the adjusted odds of 30-day readmissions by age group and insurance categories. Cost and discharge estimates were weighted per NRD procedures to reflect a nationally representative sample. Diagnoses for index hospitalizations leading to rehospitalization were determined. Among 12,533,551 discharges, 1,818,093 (14.5%) resulted in readmission within 30 days. Medicaid insurance was associated with the highest adjusted odds ratio (AOR) for readmission both in those ≥65 years old (AOR 1.12, 95%CI 1.10-1.14; p <0.001), and 45-64 (AOR 1.67, 95% CI 1.66-1.69; p < 0.001), and Medicare in the 18-44 group (Medicare vs. private insurance: AOR 1.99, 95% CI 1.96-2.01; p <0.001). Discharges for psychiatric or substance abuse disorders, septicemia, and heart failure accounted for the largest numbers of readmissions, with readmission rates of 24.0%, 17.9%, 22.9% respectively. Total costs for readmissions were 50.7 billion USD, highest for Medicare (29.6 billion USD), with non-Medicare costs exceeding 21 billion USD. While Medicare readmissions account for more than half of the total burden of readmissions, costs of non-Medicare readmissions are nonetheless substantial. Medicaid patients have the highest odds of readmission in individuals older than age 44, commonly due to hospitalizations for psychiatric illness and substance abuse disorders. Medicaid patients represent a population at uniquely high risk for readmission.
很少有研究调查不同年龄和保险类型的成年人短期再入院率及原因。我们比较了美国不同保险类型的全因住院后30天再入院率、特征和费用。我们回顾性评估了2013年1月1日至2013年11月31日期间,全国再入院数据库中21个州的2006家非联邦医院中因任何原因出院的18岁及以上存活患者。主要的分层变量是主要保险。根据行政计费代码定义的埃利克斯豪泽共病情况评估合并症。其他指标包括导致再次住院的首次住院诊断。使用以医院地点为随机效应的分层多变量逻辑回归模型,计算不同年龄组和保险类别的30天再入院调整后比值比。成本和出院估计数根据NRD程序进行加权,以反映具有全国代表性的样本。确定了导致再次住院的首次住院诊断。在12533551例出院病例中,1818093例(14.5%)在30天内再次入院。医疗补助保险与65岁及以上人群(调整后比值比[AOR]为1.12,95%置信区间[CI]为1.10 - 1.14;p < 0.001)和45 - 64岁人群(AOR为1.67,95% CI为1.66 - 1.69;p < 0.001)的再入院调整后比值比最高相关,而在18 - 44岁组中,医疗保险与再入院相关(医疗保险与私人保险相比:AOR为1.99,95% CI为1.96 - 2.01;p < 0.001)。精神疾病或药物滥用障碍、败血症和心力衰竭导致的出院病例再入院人数最多,再入院率分别为24.0%、17.9%、22.9%。再入院的总成本为507亿美元,医疗保险的成本最高(296亿美元),非医疗保险成本超过210亿美元。虽然医疗保险再入院占再入院总负担的一半以上,但非医疗保险再入院的成本仍然很高。44岁以上人群中,医疗补助患者的再入院几率最高,通常是由于精神疾病和药物滥用障碍住院。医疗补助患者是再入院风险特别高的人群。