Department of Pediatric Oncology - Hematology, VU University Medical Center, Amsterdam, The Netherlands.
Department of Clinical Pharmacology & Pharmacy, VU University Medical Center, Amsterdam, The Netherlands.
J Neurooncol. 2017 Nov;135(2):307-315. doi: 10.1007/s11060-017-2575-9. Epub 2017 Jul 26.
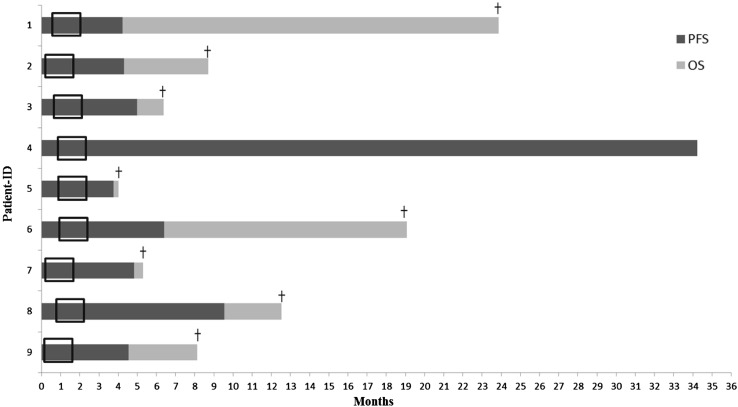
The purpose of this phase I/II, open-label, single-arm trial is to investigate the safety, tolerability, maximum tolerated dose and preliminary efficacy of the potential radiosensitizer gemcitabine, administered concomitantly to radiotherapy, in children with newly diagnosed diffuse intrinsic pontine glioma (DIPG). Six doses of weekly gemcitabine were administered intravenously, concomitantly to 6 weeks of hyperfractionated radiotherapy. Successive cohorts received increasing doses of 140, 175 and 200 mg/m gemcitabine, respectively, following a 3 + 3 dose-escalation schedule without expansion cohort. Dose-limiting toxicities (DLT) were monitored during treatment period. Clinical response was assessed using predefined case report forms and radiological response was assessed using the modified RANO criteria. Quality of life (QoL) was assessed using PedsQL questionnaires. Between June 2012 and December 2016, nine patients were enrolled. Treatment was well tolerated, and no DLTs were observed up to the maximum dose of 200 mg/m. All patients experienced reduction of tumor-related symptoms. QoL tended to improve during treatment. PFS and MOS were 4.8 months (95% CI 4.0-5.7) and 8.7 months (95% CI 7.0-10.4). Classifying patients according to the recently developed DIPG survival prediction model, intermediate risk patients (n = 4), showed a PFS and MOS of 6.4 and 12.4 months, respectively, versus a PFS and MOS of 4.5 and 8.1 months, respectively, in high risk patient (n = 5). Gemcitabine up to 200 mg/m/once weekly, added to radiotherapy, is safe and well tolerated in children with newly diagnosed DIPG. PFS and MOS were not significantly different from literature.
本 I/II 期、开放性、单臂试验的目的是研究新诊断的弥漫性内在脑桥神经胶质瘤(DIPG)儿童同时接受放射治疗时,潜在放射增敏剂吉西他滨的安全性、耐受性、最大耐受剂量和初步疗效。每周静脉注射 6 剂吉西他滨,与 6 周的超分割放射治疗同时进行。根据 3+3 剂量递增方案,在没有扩展队列的情况下,分别连续接受递增剂量的 140、175 和 200mg/m 吉西他滨。在治疗期间监测剂量限制性毒性(DLT)。使用预设的病例报告表评估临床反应,使用改良的 RANO 标准评估放射学反应。使用 PedsQL 问卷评估生活质量(QoL)。2012 年 6 月至 2016 年 12 月,共纳入 9 例患者。治疗耐受性良好,最大剂量 200mg/m 时未观察到 DLT。所有患者均经历肿瘤相关症状减轻。治疗期间 QoL 趋于改善。PFS 和 MOS 分别为 4.8 个月(95%CI 4.0-5.7)和 8.7 个月(95%CI 7.0-10.4)。根据最近开发的 DIPG 生存预测模型对患者进行分类,中间风险患者(n=4)的 PFS 和 MOS 分别为 6.4 和 12.4 个月,而高风险患者(n=5)的 PFS 和 MOS 分别为 4.5 和 8.1 个月。每周一次、剂量高达 200mg/m 的吉西他滨,联合放疗,在新诊断的 DIPG 儿童中是安全且耐受良好的。PFS 和 MOS 与文献报道无显著差异。