Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy.
Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy.
Eur Urol Focus. 2019 Mar;5(2):242-249. doi: 10.1016/j.euf.2017.05.006. Epub 2017 Jun 3.
Limited data is available on the role, and extent of, postchemotherapy lymphadenectomy (PC-LND) in patients with clinical evidence of pelvic (cN1-3) or retroperitoneal (RP) lymph node spread from urothelial bladder carcinoma.
To compare the outcomes of operated versus nonoperated patients after first-line chemotherapy.
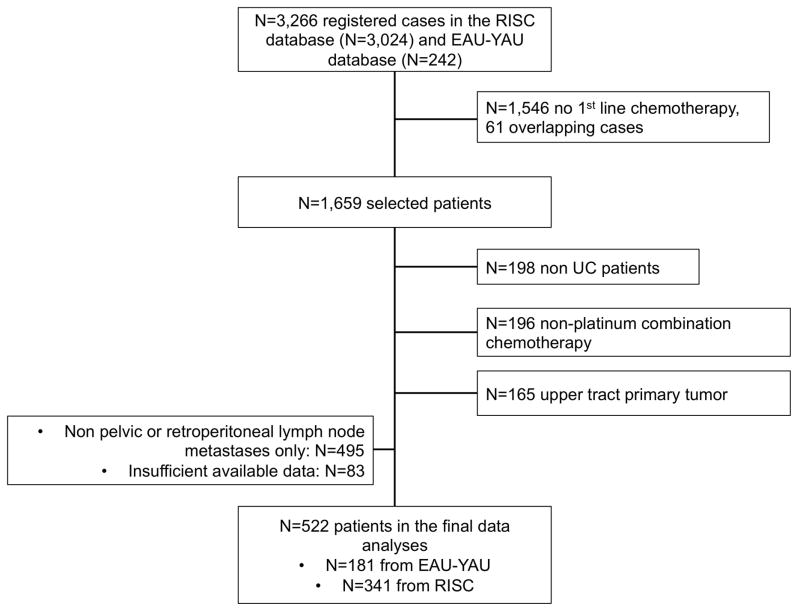
DESIGN, SETTING, AND PARTICIPANTS: Data from 34 centers was collected, totaling 522 patients, treated between January 2000 and June 2015. Criteria for patient selection were the following: bladder primary tumor, lymph node metastases (pelvic±RP) only, first-line platinum-based chemotherapy given.
LND (with cystectomy) versus observation after first-line chemotherapy for metastatic urothelial bladder carcinoma.
Overall survival (OS) was the primary endpoint. Multiple propensity score techniques were adopted, including 1:1 propensity score matching and inverse probability of treatment weighting. Additionally, the inverse probability of treatment weighting analysis was performed with the inclusion of the covariates, that is, with doubly robust estimation.
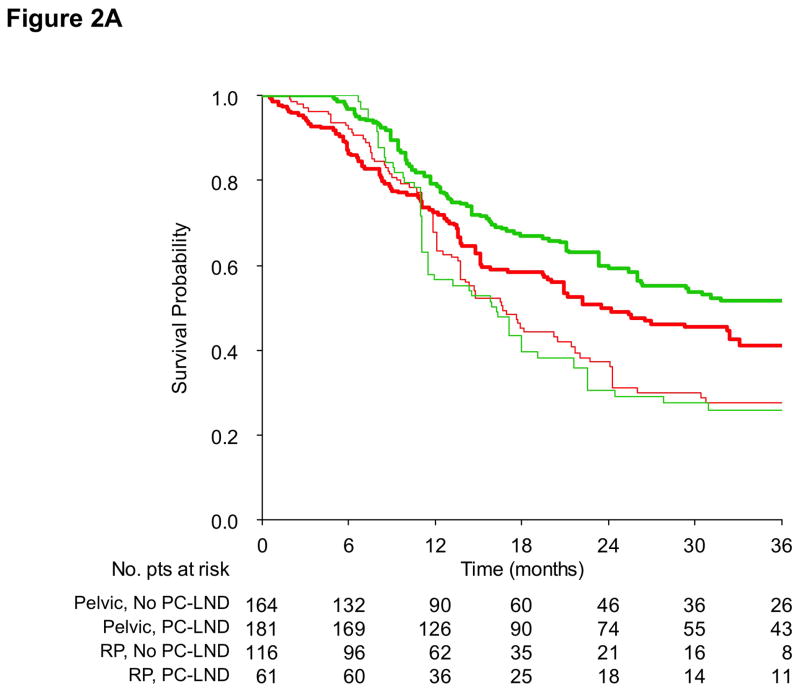
Overall, 242 (46.4%) patients received PC-LND and 280 (53.6%) observation after chemotherapy. There were 177 (33.9%) and 345 (66.1%) patients with either RP or pelvic LND only, respectively. Doubly robust estimation-adjusted comparison was not significant for improved OS for PC-LND (hazard ratio [HR]: 0.86, 95% confidence interval [CI]: 0.56-1.31, p=0.479), confirmed by matched analysis (HR: 0.91, 95% CI: 0.60-1.36, p=0.628). This was also observed in the RP subgroup (HR: 1.12, 95% CI: 0.68-1.84). The retrospective nature of the data and the heterogeneous patient population were the major limitations.
Although there were substantial differences between the two groups, after accounting for major confounders we report a nonsignificant OS difference with PC-LND compared with observation only. These findings may be hypothesis-generating for future prospective trials.
We found no differences in survival by adding postchemotherapy lymphadenectomy in patients with pelvic or retroperitoneal lymph node metastatic bladder cancer. The indication to perform postchemotherapy lymphadenectomy in the most suitable patients requires additional studies.
在有盆腔(cN1-3)或腹膜后(RP)淋巴结转移的临床证据的尿路上皮膀胱癌患者中,化疗后淋巴结切除术(PC-LND)的作用和范围的数据有限。
比较一线化疗后手术与非手术患者的结局。
设计、地点和参与者:收集了 34 个中心的数据,共 522 名患者,他们于 2000 年 1 月至 2015 年 6 月接受治疗。患者选择标准如下:膀胱原发性肿瘤,仅淋巴结转移(盆腔±RP),一线铂类化疗。
转移性尿路上皮膀胱癌一线化疗后行 LND(伴膀胱切除术)或观察。
总生存(OS)是主要终点。采用了多种倾向评分技术,包括 1:1 倾向评分匹配和治疗反概率加权。此外,还进行了治疗反概率加权分析,并纳入了协变量,即双重稳健估计。
总体而言,242 名(46.4%)患者接受了 PC-LND,280 名(53.6%)患者在化疗后接受了观察。分别有 177 名(33.9%)和 345 名(66.1%)患者仅行 RP 或盆腔 LND。经双重稳健估计校正后的 OS 比较显示,PC-LND 并未显著改善(风险比[HR]:0.86,95%置信区间[CI]:0.56-1.31,p=0.479),匹配分析结果也证实了这一点(HR:0.91,95%CI:0.60-1.36,p=0.628)。在 RP 亚组也观察到同样的结果(HR:1.12,95%CI:0.68-1.84)。数据的回顾性和患者人群的异质性是主要的局限性。
尽管两组之间存在显著差异,但在考虑了主要混杂因素后,我们报告 PC-LND 与单纯观察相比,OS 无显著差异。这些发现可能为未来的前瞻性试验提供假设。
我们发现,在盆腔或腹膜后淋巴结转移性膀胱癌患者中,化疗后行淋巴结切除术并不能提高生存率。在最合适的患者中进行化疗后淋巴结切除术的适应证还需要进一步的研究。