Moore Hunter B, Moore Ernest E, Huebner Benjamin R, Stettler Gregory R, Nunns Geoffrey R, Einersen Peter M, Silliman Christopher C, Sauaia Angela
Department of Surgery, University of Colorado Denver, Aurora, Colorado.
Department of Surgery, University of Colorado Denver, Aurora, Colorado; Department of Surgery, Denver Health Medical Center, Denver, Colorado.
J Surg Res. 2017 Dec;220:438-443. doi: 10.1016/j.jss.2017.04.028. Epub 2017 May 8.
Tranexamic acid (TXA) administration after trauma has not been proven to improve survival in the United States. Trauma patients were presented to the hospital with a spectrum of fibrinolytic activity, in which physiological levels of fibrinolysis are associated with the lowest mortality. We hypothesize that trauma patients who present to the hospital with physiological levels of fibrinolysis will have increased mortality if they receive TXA.
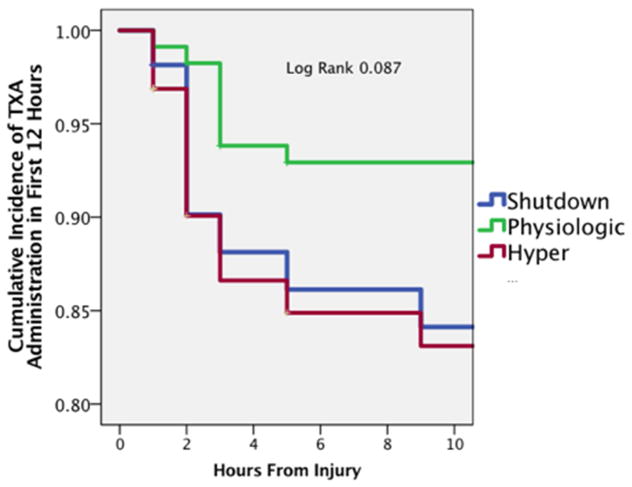
Severely injured trauma patients, followed prospectively from 2014 to 2016, were included in the analysis. The patient's first thrombelastography was used to stratify patients into fibrinolysis phenotypes which included fibrinolysis shutdown, physiological fibrinolysis, and systemic hyperfibrinolysis. The primary outcome was in-hospital mortality.
A total of 232 patients were analyzed (11% received TXA) with an overall mortality rate of 20%. TXA administration was associated with a higher new injury severity score (49 versus 28; P = 0.001), massive transfusion rate (69% versus 12%; P < 0.001), and mortality (52% versus 17%; P < 0.001). Hyperfibrinolysis and shutdown had higher mortality rates than physiological group (24% versus 30% versus 14%; P = 0.050). The effect of TXA within phenotypes was not significant for shutdown (28% versus 38%; P = 0.604) but was significant in the physiological group (11% versus 63%; P < 0.001) and systemic hyperfibrinolysis (19% versus 55%; P = 0.023). After adjusting for new injury severity score, TXA remained a significant predictor of mortality for patients with physiological fibrinolysis (P = 0.018).
There was no clear benefit of receiving TXA in this study, and patients who present to the hospital with physiologic levels of fibrinolysis, who received TXA, had the highest mortality. The role of TXA in mature trauma systems remains unclear, and emerging data supports it may have adverse effects.
在美国,创伤后使用氨甲环酸(TXA)尚未被证明能提高生存率。创伤患者入院时具有一系列纤溶活性,其中生理水平的纤溶与最低死亡率相关。我们假设,入院时具有生理水平纤溶的创伤患者若接受TXA,死亡率将会增加。
分析2014年至2016年前瞻性随访的严重创伤患者。患者的首次血栓弹力图用于将患者分层为纤溶表型,包括纤溶关闭、生理纤溶和全身高纤溶。主要结局是院内死亡率。
共分析了232例患者(11%接受了TXA),总体死亡率为20%。使用TXA与更高的新损伤严重程度评分(49对28;P = 0.001)、大量输血率(69%对12%;P < 0.001)和死亡率(52%对17%;P < 0.001)相关。高纤溶和纤溶关闭组的死亡率高于生理组(24%对30%对14%;P = 0.050)。TXA在各表型中的作用在纤溶关闭组不显著(28%对38%;P = 0.604),但在生理组显著(11%对63%;P < 0.001),在全身高纤溶组也显著(19%对55%;P = 0.023)。在调整新损伤严重程度评分后,TXA仍然是生理纤溶患者死亡率的显著预测因素(P = 0.018)。
本研究中接受TXA没有明显益处,入院时具有生理纤溶水平且接受TXA的患者死亡率最高。TXA在成熟创伤系统中的作用仍不明确,新出现的数据支持其可能有不良反应。