Higashiya Shunichi, Yamaji Hirosuke, Murakami Takashi, Hina Kazuyoshi, Kawamura Hiroshi, Murakami Masaaki, Kamikawa Shigeshi, Komatsubara Issei, Kusachi Shozo
Heart Rhythm Center, Okayama Heart Clinic, Okayama, Japan.
Department of General Internal Medicine, Kawasaki Hospital, Kawasaki Medical School, Okayama, Japan.
Open Heart. 2017 Mar 27;4(1):e000593. doi: 10.1136/openhrt-2017-000593. eCollection 2017.
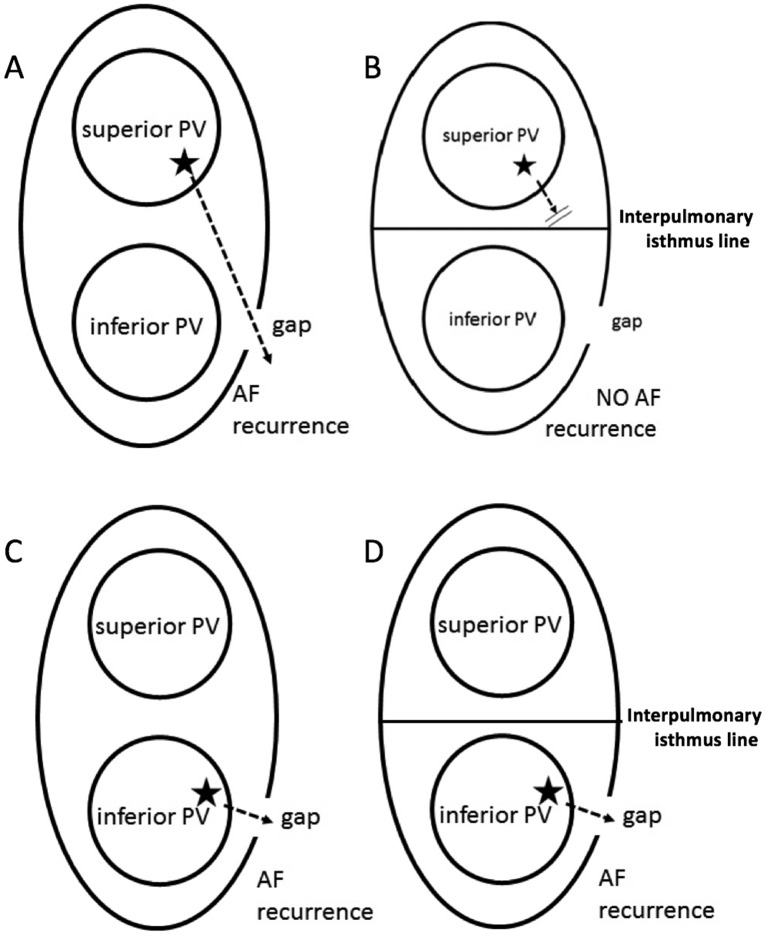
Data on the efficacy of adjunctive interpulmonary isthmus ablation following completion of extensive encircling pulmonary vein isolation (EEPVI) on atrial fibrillation (AF) recurrence have still been insufficient. We aimed to compare the AF recurrence between EEPVI with and without adjunctive interpulmonary isthmus ablation.
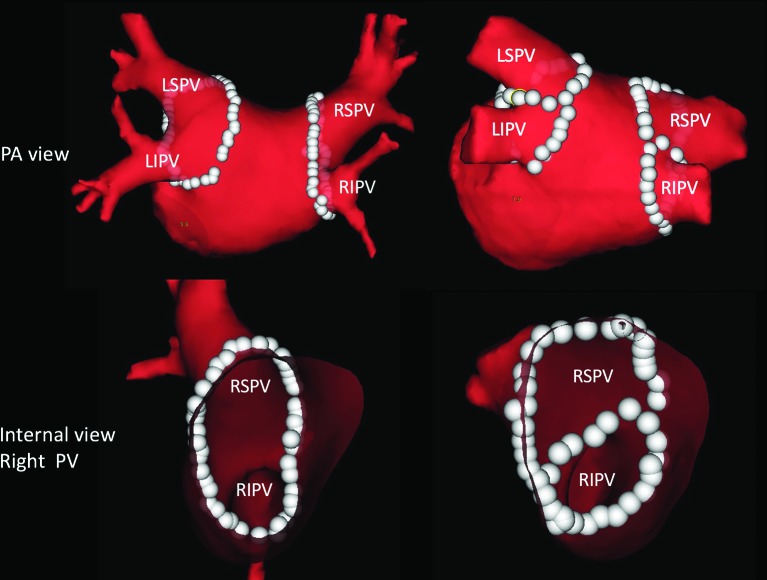
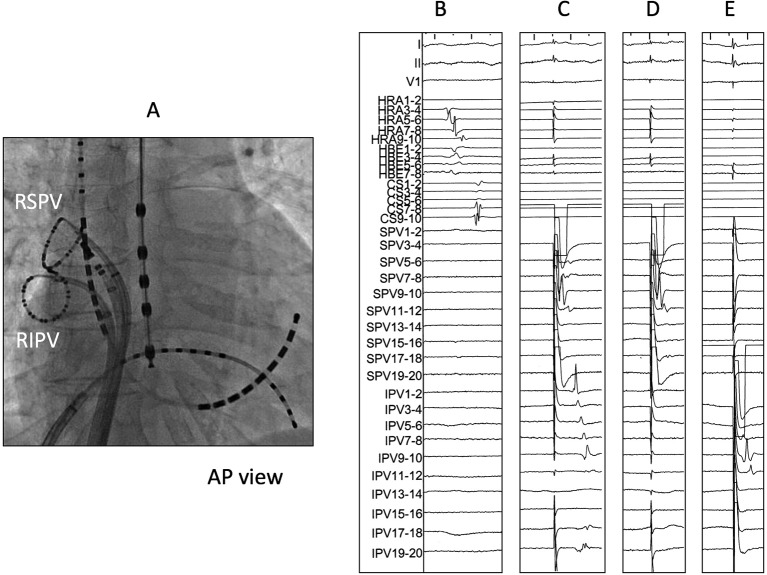
We enrolled 200 consecutive patients with paroxysmal AF (first session) who underwent EEPVI with double-Lasso technique. Patients were prospectively randomised into two groups: EEPVI with (group 1) and without (group 2) adjunctive interpulmonary isthmus ablation.
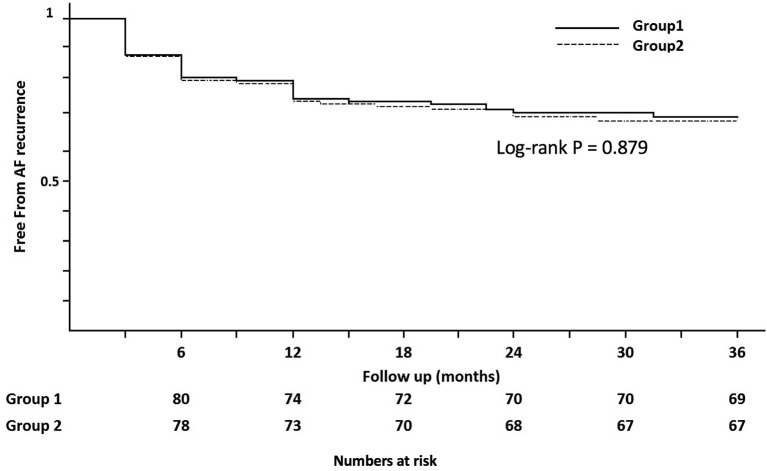
No differences were found in patients' clinical and echocardiographic backgrounds, including arrhythmia status, between the two groups. No differences were also observed in complications (two groin haematoma in both groups). All patients in both groups reached the EEPVI endpoint. The AF recurrence rate between groups 1 (32/100, 32%) and 2 (33/100, 33%; p=1.0) was quite similar during the follow-up period (45±5 months; 36-54 months). The two groups showed identical Kaplan-Meier AF-free curves (p=0.460; NS). Similar pulmonary vein (PV) reconnection incidence was observed in both groups during the second session. Durable isolation between the superior and inferior PVs was confirmed in 88% (21/27) of patients in group 1, indicating that interpulmonary isthmus ablation maintained a non-conducting state in a considerable number of patients. Nevertheless, AF recurrence was identical between the two groups.
The results of our study showed similar AF recurrence rates between the two groups, indicating that adjunctive interpulmonary isthmus ablation with EEPVI has no obvious effects on AF recurrence.
关于在完成广泛环绕肺静脉隔离(EEPVI)后进行肺内峡部附加消融对房颤(AF)复发疗效的数据仍然不足。我们旨在比较进行和未进行肺内峡部附加消融的EEPVI患者的房颤复发情况。
我们纳入了200例连续的阵发性房颤患者(首次发作),这些患者接受了双套索技术的EEPVI。患者被前瞻性随机分为两组:进行肺内峡部附加消融的组1和未进行的组2。
两组患者的临床和超声心动图背景,包括心律失常状态,均无差异。并发症方面(两组均有两例腹股沟血肿)也未观察到差异。两组所有患者均达到EEPVI终点。在随访期(45±5个月;36 - 54个月)内,组1(32/100,32%)和组2(33/100,33%;p = 1.0)的房颤复发率相当相似。两组的Kaplan - Meier无房颤曲线相同(p = 0.460;无显著性差异)。在第二次手术期间,两组观察到相似的肺静脉(PV)重新连接发生率。组1中88%(21/27)的患者证实上、下肺静脉之间实现了持久隔离,表明肺内峡部消融在相当数量的患者中维持了非传导状态。然而,两组的房颤复发情况相同。
我们的研究结果显示两组的房颤复发率相似,表明EEPVI联合肺内峡部附加消融对房颤复发没有明显影响。