Letsas Konstantinos P, Georgopoulos Stamatis, Efremidis Michael, Liu Tong, Bazoukis George, Vlachos Konstantinos, Karamichalakis Nikolaos, Lioni Louiza, Sideris Antonios, Ehrlich Joachim R
Laboratory of Cardiac Electrophysiology, "Evangelismos" General Hospital of Athens, Greece.
Department of Cardiology, Tianjin Institute of Cardiology, Second Hospital of Tianjin Medical University, People׳s Republic of China.
J Arrhythm. 2017 Aug;33(4):247-255. doi: 10.1016/j.joa.2017.02.002. Epub 2017 Mar 28.
The prognostic significance of adenosine-mediated dormant pulmonary vein conduction, and whether such dormant conduction should be eliminated, remains controversial. We sought to perform a meta-analysis of data from eligible studies to delineate the prognostic impact of adenosine-guided radiofrequency catheter ablation of atrial fibrillation.
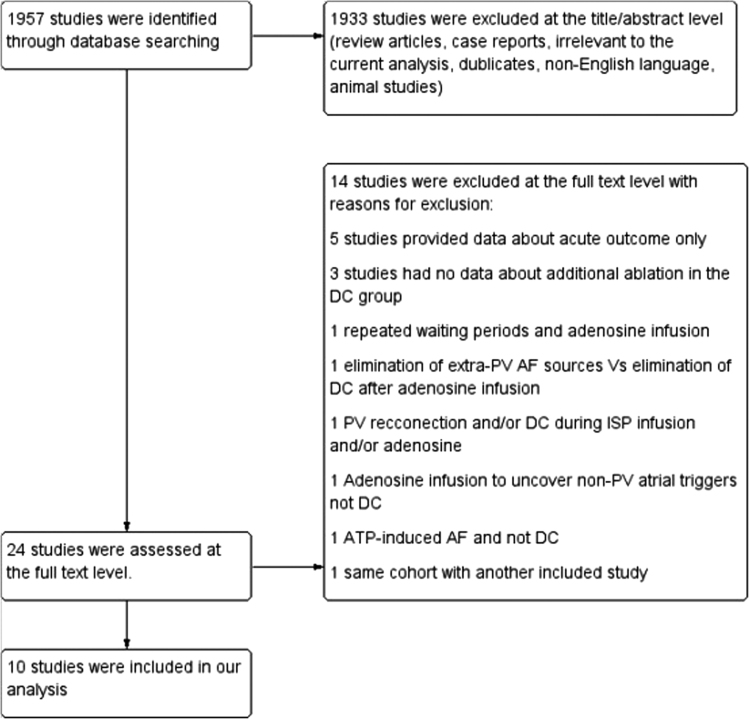
A systematic literature search was performed using online databases in order to identify relevant studies from January 2004 to September 2016. Ten studies [six observational and four randomized control trials (RCTs)] were included in the analysis.
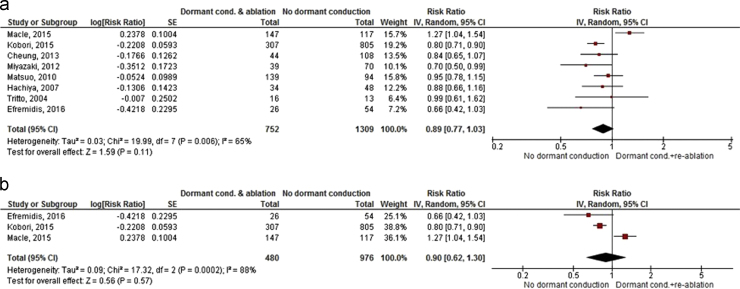
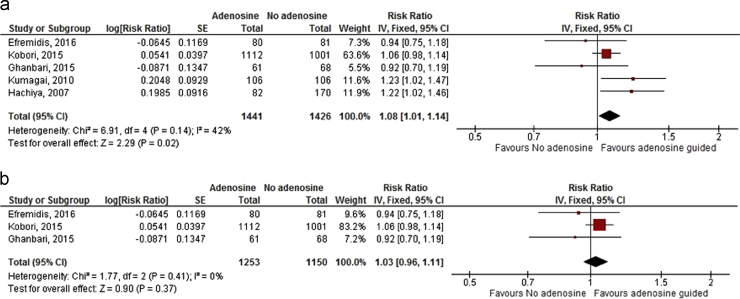
Five studies (two observational and three RCTs) compared the efficacy of adenosine-mediated elimination of dormant conduction versus no adenosine test. Overall, the adenosine-guided ablation strategy displayed better long-term outcomes as compared with no adenosine testing (RR 1.08, 95% CI 1.01-1.14, =0.02; Heterogeneity: =42%, : 0.14). The meta-analysis of only RCTs failed to show any differences between the two strategies (RR 1.03, 95% CI 0.96-1.11, =0.37; Heterogeneity: 0%, : 0.41). Eight studies (five observational and three RCTs) addressed the efficacy of adenosine-induced dormant conduction and additional ablation versus no dormant conduction during adenosine challenge. Overall, a trend towards a better outcome in those without dormant conduction during drug challenge was noted (RR 0.89, 95% CI 0.77-1.03, =0.11; Heterogeneity: 65% : 0.006). The pooled analysis of RCTs failed to show any differences between the two arms (RR 0.90, 95% CI 0.62-1.30, = 0.57; Heterogeneity: 88%, : 0.0002).
Adenosine-guided radiofrequency catheter ablation of atrial fibrillation does not provide additional benefit in terms of freedom of arrhythmia recurrence.
腺苷介导的隐匿性肺静脉传导的预后意义以及是否应消除这种隐匿性传导仍存在争议。我们试图对符合条件的研究数据进行荟萃分析,以明确腺苷指导下的房颤射频导管消融术的预后影响。
利用在线数据库进行系统的文献检索,以识别2004年1月至2016年9月的相关研究。分析纳入了10项研究[6项观察性研究和4项随机对照试验(RCT)]。
5项研究(2项观察性研究和3项RCT)比较了腺苷介导消除隐匿性传导与不进行腺苷试验的疗效。总体而言,与不进行腺苷试验相比,腺苷指导的消融策略显示出更好的长期结果(RR 1.08,95%CI 1.01-1.14,P = 0.02;异质性:I² = 42%,P = 0.14)。仅对RCT进行的荟萃分析未显示两种策略之间存在任何差异(RR 1.03,95%CI 0.96-1.11,P = 0.37;异质性:I² = 0%,P = 0.41)。8项研究(5项观察性研究和3项RCT)探讨了腺苷诱发隐匿性传导及额外消融与腺苷激发试验期间无隐匿性传导的疗效。总体而言,注意到药物激发试验期间无隐匿性传导者有更好结局的趋势(RR 0.89,95%CI 0.77-1.03,P = 0.11;异质性:I² = 65%,P = 0.006)。RCT的汇总分析未显示两组之间存在任何差异(RR 0.90,95%CI 0.62-1.30,P = 0.57;异质性:I² = 88%,P = 0.0002)。
腺苷指导的房颤射频导管消融术在心律失常复发自由度方面未提供额外益处。