Papatheodoridi Μargarita, Dalekos George N, Goulis John, Manolakopoulos Spilios, Triantos Christos, Zachou Kalliopi, Koukoufiki Argyro, Κourikou Αnastasia, Ζisimopoulos Κonstantinos, Τsoulas Christos, Papatheodoridis George V
Department of Gastroenterology, Medical School of National and Kapodistrian University of Athens, Laiko General Hospital, Athens (Margarita Papatheodoridi, George V. Papatheodoridis), Greece.
Department of Medicine and Research Laboratory of Internal Medicine, Thessaly University Medical School, Larissa, Greece (George N. Dalekos, Kalliopi Zachou), Greece.
Ann Gastroenterol. 2017;30(5):542-549. doi: 10.20524/aog.2017.0170. Epub 2017 Jun 26.
We determined the proportions of patients with chronic hepatitis C (CHC) in association with possible prioritized indications for interferon-free regimens and the use of co-medications with potential drug-drug interactions (DDIs).
Five hundred consecutive mono-infected CHC patients seen in 2015 at 5 Greek centers were included. Priorities for interferon-free regimens were based on liver disease severity, contraindication(s) for interferon and prior interferon-treatment failure. All co-medications were classified into those with no DDIs/no clear data for DDIs, potential DDIs, and contraindication due to DDI for each agent, according to the HEP Drug Interaction Checker.
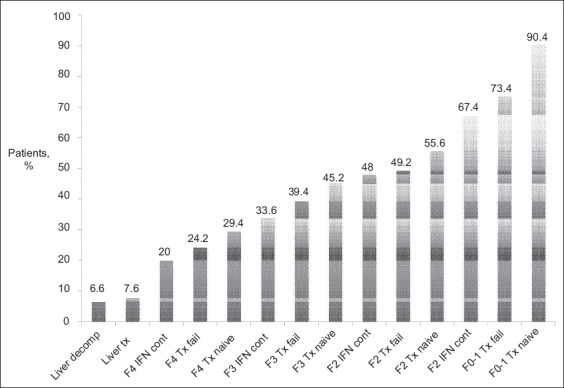
Of the 500 patients, 1% had undergone liver transplantation, whereas 6.6% had decompensated cirrhosis, 21.8% F4, 17.1% F3, 10.4% F2, and 34.8% F0-1 fibrosis. Contraindications for interferon were present in 38.5% of non-transplant patients with compensated liver disease. The probability of contraindications/potential DDIs was greater for boceprevir/telaprevir and ombitasvir/paritaprevir/ritonavir±dasabuvir, compared to all other agents (P<0.001), and least for sofosbuvir (P<0.05). Contraindications/potential DDIs were more frequently present in patients ≥50 than <50 years old (P≤0.034), and more common in F3-4 than F0-2, and F4 than F0-3 fibrosis (P≤0.019) for all direct-acting antivirals (DAAs).
The expansion of the criteria for prioritization of interferon-free regimens from cirrhosis to F3 and perhaps F2 fibrosis will increase the proportion of patients with DAA access by only 10-15% and 10%, respectively. A potential for DDIs is frequently present with protease inhibitors, but also exists with other DAAs. The probability of DDIs is higher in patients with priority for DAAs, including those who have advanced liver disease and are usually of older age.
我们确定了慢性丙型肝炎(CHC)患者中与无干扰素治疗方案可能的优先指征相关的比例,以及使用存在潜在药物相互作用(DDIs)的联合用药情况。
纳入2015年在希腊5个中心就诊的500例连续的单感染CHC患者。无干扰素治疗方案的优先级基于肝病严重程度、干扰素禁忌症和既往干扰素治疗失败情况。根据HEP药物相互作用检查器,将所有联合用药分为无DDIs/无DDIs明确数据、潜在DDIs以及因DDIs导致禁忌症的药物。
500例患者中,1%接受过肝移植,6.6%有失代偿性肝硬化,21.8%为F4,17.1%为F3,10.4%为F2,34.8%为F0-1纤维化。在有代偿性肝病的非移植患者中,38.5%存在干扰素禁忌症。与所有其他药物相比,博赛匹韦/特拉匹韦以及奥比他韦/帕立普韦/利托那韦±达沙布韦出现禁忌症/潜在DDIs的可能性更大(P<0.001),而索磷布韦的可能性最小(P<0.05)。对于所有直接抗病毒药物(DAA),≥50岁患者出现禁忌症/潜在DDIs的频率高于<50岁患者(P≤0.034),在F3-4纤维化患者中比F0-2纤维化患者更常见,在F4纤维化患者中比F0-3纤维化患者更常见(P≤0.019)。
将无干扰素治疗方案的优先标准从肝硬化扩大到F3级甚至可能F2级纤维化,分别只会使有机会使用DAA的患者比例增加10%-15%和10%。蛋白酶抑制剂常常存在潜在DDIs的可能性,但其他DAA也存在这种情况。在有DAA使用优先级的患者中,包括那些患有晚期肝病且通常年龄较大的患者,出现DDIs的可能性更高。