Chen Jinbin, Huang Jia, Chen Minshan, Yang Keli, Chen Jiancong, Wang Juncheng, Xu Li, Zhou Zhongguo, Zhang Yaojun
Department of Hepatobiliary Surgery, Sun Yat-sen University Cancer Center, 651 Dongfeng Road East, Guangzhou 510060, China.
Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, China.
J Cancer. 2017 Aug 25;8(15):2984-2991. doi: 10.7150/jca.20978. eCollection 2017.
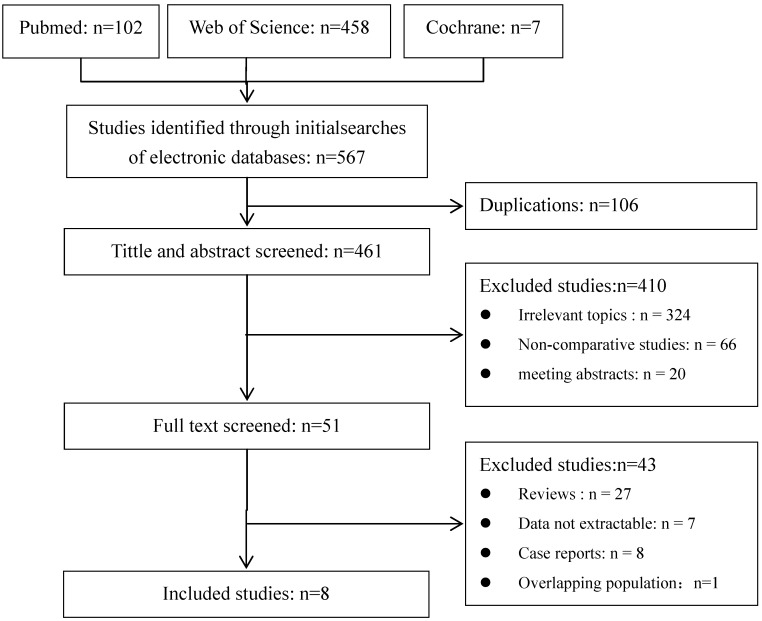
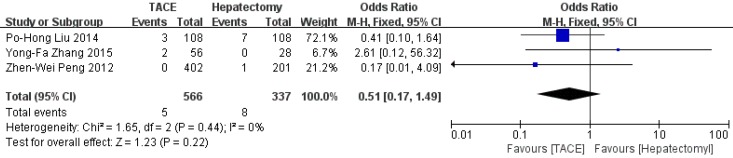
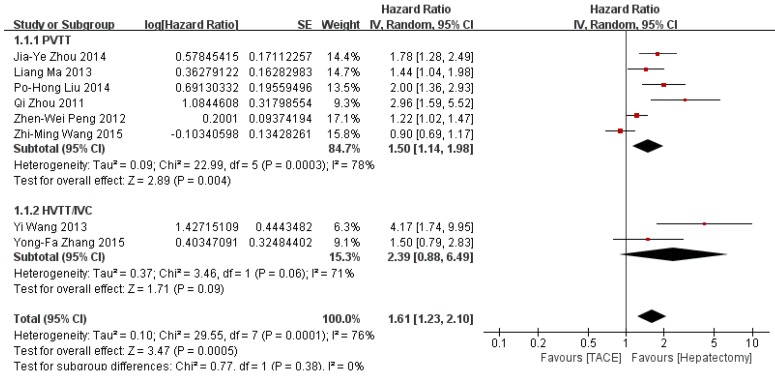
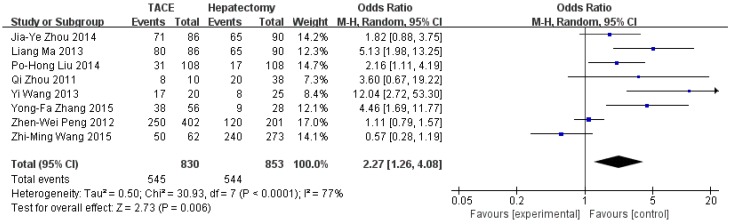
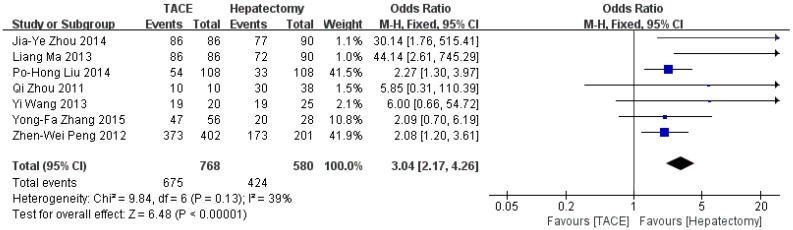
For hepatocellular carcinoma (HCC) patients with macrovascular invasion (MaVI), hepatectomy and transcatheter arterial chemoembolization (TACE) remain the main treatment options in Asia. However, which could achieve better survivals remains controversial. In present study, we conducted a meta-analysis to clarify the survival benefits and safety of hepatectomy versus TACE in HCC patients with MaVI. The PubMed, Cochrane Library and Web of Science databases were searched for eligible studies. There were no prospective studies identified. 8 retrospective studies from Asia with 1683 patients met our inclusion criteria were included in meta-analysis. The overall survival (OS) is higher in hepatectomy group than TACE group (HR=1.61, 95%CI=1.23-2.10, =0.0005). Hepatectomy was superior over TACE in 1-year (OR=2.27, 95%CI=1.26-4.08, =0.006) and 3-year (OR=3.04, 95%CI=2.17-4.26, <0.00001) respectively, but not in 5-year (OR=7.34, 95%CI=0.78-68.16, =0.08) survival rate. Subgroup analysis demonstrated that hepatectomy was superior over TACE for patients with PVTT (HR=1.50, 95%CI=1.14-1.98, =0.004), but not for patients with HVTT/IVC (HR=2.39, 95%CI=0.88-6.49, =0.09). There was not significantly difference between two groups in peri-operative mortality. Our results indicated that, compared to TACE, hepatectomy might be a better treatment option for resectable HCC patients with MaVI. Being lack of high-quality studies, more well-designed multi-center randomized trials are needed to confirm our finding.
对于伴有大血管侵犯(MaVI)的肝细胞癌(HCC)患者,肝切除术和经动脉化疗栓塞术(TACE)仍是亚洲的主要治疗选择。然而,哪种方法能带来更好的生存率仍存在争议。在本研究中,我们进行了一项荟萃分析,以阐明肝切除术与TACE在伴有MaVI的HCC患者中的生存获益和安全性。我们检索了PubMed、Cochrane图书馆和科学网数据库以查找符合条件的研究。未检索到前瞻性研究。来自亚洲的8项回顾性研究共1683例患者符合纳入标准并纳入荟萃分析。肝切除组的总生存期(OS)高于TACE组(HR = 1.61,95%CI = 1.23 - 2.10,P = 0.0005)。肝切除术在1年(OR = 2.27,95%CI = 1.26 - 4.08,P = 0.006)和3年(OR = 3.04,95%CI = 2.17 - 4.26,P < 0.00001)生存率方面优于TACE,但在5年生存率方面并非如此(OR = 7.34,95%CI = 0.78 - 68.16,P = 0.08)。亚组分析表明,肝切除术对于门静脉癌栓(PVTT)患者优于TACE(HR = 1.50,95%CI = 1.14 - 1.98,P = 0.004),但对于肝静脉/下腔静脉癌栓(HVTT/IVC)患者并非如此(HR = 2.39,95%CI = 0.88 - 6.49,P = 0.09)。两组围手术期死亡率无显著差异。我们的结果表明,与TACE相比,肝切除术可能是伴有MaVI的可切除HCC患者更好的治疗选择。由于缺乏高质量研究,需要更多设计良好的多中心随机试验来证实我们的发现。