Dellaportas Dionysios, Arkadopoulos Nikolaos, Tzanoglou Ioannis, Bairamidis Evgenios, Gemenetzis George, Xanthakos Pantelis, Nastos Constantinos, Kostopanagiotou Georgia, Vassiliou Ioannis, Smyrniotis Vassilios
2nd Department of Surgery, Aretaieion University Hospital, University of Athens School of Medicine, Athens, Greece.
4th Department of Surgery, Attikon University Hospital, University of Athens School of Medicine, Athens, Greece.
Front Surg. 2017 Sep 6;4:48. doi: 10.3389/fsurg.2017.00048. eCollection 2017.
Renal vein or inferior vena cava (IVC) invasion by neoplastic thrombus in patients with renal cell carcinoma (RCC) is not an obstacle for radical oncological treatment. The aim of this study is to present our technical maneuvers for complete removal of the intracaval thrombus without compromising hemodymanic stability of the patient.
Between 2000 and 2014, 15 RCC patients with IVC involvement of levels I-III were treated with curative intent and were prospectively studied. The operative technique varied according to thrombus extent. For type I, extraction of the thrombus is facilitated by a 2-3 cm longitudinal incision on the IVC that begins at the level of the renal vein and extends cranially, encompassing a vessel wall rim of the orifice of the resected renal vein. For type II cases, the IVC is clamped above the neoplastic thrombus, and for type III, the IVC clamping is combined with hepatic blood flow control with "Pringle maneuver." For type IV, the IVC is clamped above the diaphragm, or if the thrombus extends into the right atrium cardiothoracic input is appropriate.
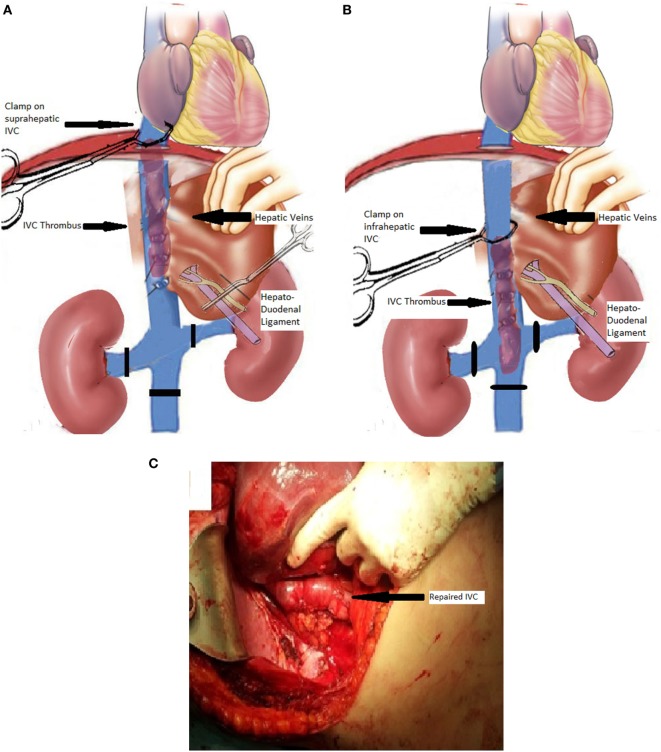
The main operative steps include preparation and control of the renal vessels and the IVC. Occasionally, for type III tumor thrombi, the patient becomes hemodynamically unstable when IVC is clamped suprahepatically. In such a case, a novel operative maneuver of milking the thrombus below the orifice of the hepatic veins, and subsequently the IVC clamp also beneath the hepatic veins, allowing release of the "Pringle maneuver" is performed. This operative step restores hepatic blood flow and hemodynamic stability and is based on the floating nature of the thrombus into the IVC. Mean operative time was 120 min (range from 90 to 180 min), and average liver and renal warm ischemia time was 20 min (range from 15 to 35 min). Postoperative overall hospital stay ranged from 7 to 13 days.
The technical solutions employed in the current study allow successful removal of neoplastic thrombi from the IVC in most cases, associated with minimal perioperative complication rate even for patients who due to multiple comorbidities would be considered otherwise inoperable.
肾细胞癌(RCC)患者出现肿瘤血栓侵犯肾静脉或下腔静脉(IVC)并非根治性肿瘤治疗的障碍。本研究的目的是介绍我们在不影响患者血液动力学稳定性的情况下完全清除腔静脉内血栓的技术操作。
2000年至2014年间,对15例I-III级IVC受累的RCC患者进行了根治性治疗,并进行了前瞻性研究。手术技术根据血栓范围而异。对于I型,通过在IVC上作一个2-3厘米的纵向切口来便于取出血栓,该切口从肾静脉水平开始并向上延伸,包括切除的肾静脉开口处的血管壁边缘。对于II型病例,在肿瘤血栓上方夹住IVC,对于III型,IVC夹闭与用“Pringle手法”控制肝血流相结合。对于IV型,在膈肌上方夹住IVC,或者如果血栓延伸至右心房,则进行心胸外科干预是合适的。
主要手术步骤包括肾血管和IVC的准备与控制。偶尔,对于III型肿瘤血栓,当在肝上方夹住IVC时患者会出现血液动力学不稳定。在这种情况下,采用一种新的手术操作,即将血栓挤到肝静脉开口下方,随后IVC夹也置于肝静脉下方,从而可以松开“Pringle手法”。这一手术步骤可恢复肝血流和血液动力学稳定性,其依据是血栓在IVC内的漂浮特性。平均手术时间为120分钟(范围为90至180分钟),平均肝脏和肾脏热缺血时间为20分钟(范围为15至35分钟)。术后总住院时间为7至13天。
本研究采用的技术方案在大多数情况下能够成功地从IVC中清除肿瘤血栓,即使对于因多种合并症而被认为无法手术的患者,围手术期并发症发生率也很低。