Katsanos Konstantinos, Kitrou Panagiotis, Spiliopoulos Stavros, Maroulis Ioannis, Petsas Theodore, Karnabatidis Dimitris
Department of Interventional Radiology, Patras University Hospital, School of Medicine, Rion, Greece.
Department of Interventional Radiology, Guy's and St. Thomas' Hospitals, NHS Foundation Trust, King's Health Partners, London, United Kingdom.
PLoS One. 2017 Sep 21;12(9):e0184597. doi: 10.1371/journal.pone.0184597. eCollection 2017.
The optimal transcatheter embolization strategy for patients with unresectable hepatocellular carcinoma (HCC) remains elusive. We conducted a systematic review and network meta-analysis (NMA) of different embolization options for unresectable HCC.
Medical databases were searched for randomized controlled trials evaluating bland transarterial embolization (TAE), conventional TACE, drug-eluting bead chemoembolization (DEB-TACE), or transarterial radioembolization (TARE), either alone or combined with adjuvant chemotherapy, or local liver ablation, or external radiotherapy for unresectable HCC up to June 2017. Random effects Bayesian models with a binomial and normal likelihood were fitted (WinBUGS). Primary endpoint was patient survival expressed as hazard ratios (HR) and 95% credible intervals. An exponential model was used to fit patient survival curves. Safety and objective response were calculated as odds ratios (OR) and accompanying 95% credible intervals. Competing treatments were ranked with the SUCRA statistic. Heterogeneity-adjusted effective sample sizes were calculated to evaluate information size for each comparison. Quality of evidence (QoE) was assessed with the GRADE system adapted for NMA reports. All analyses complied with the ISPOR-AMCP-NCP Task Force Report for good practice in NMA.
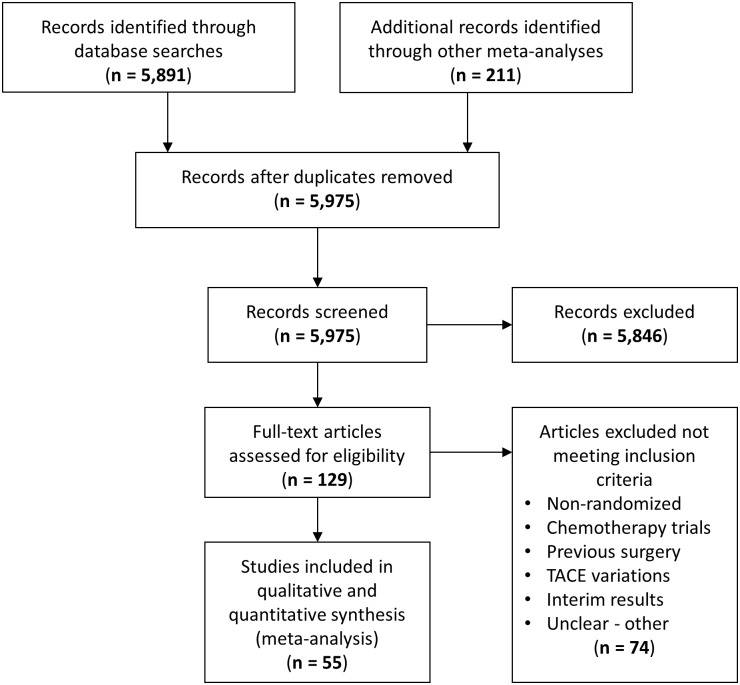
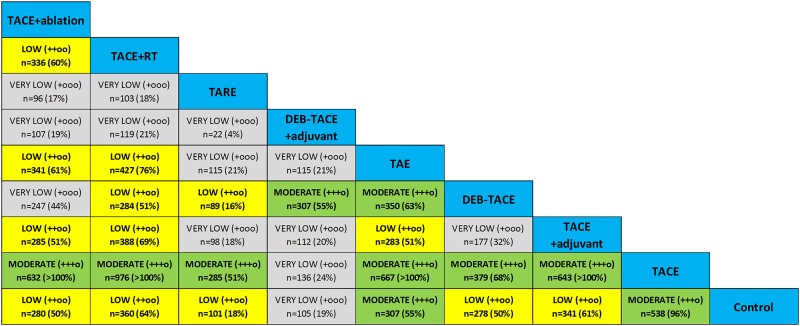
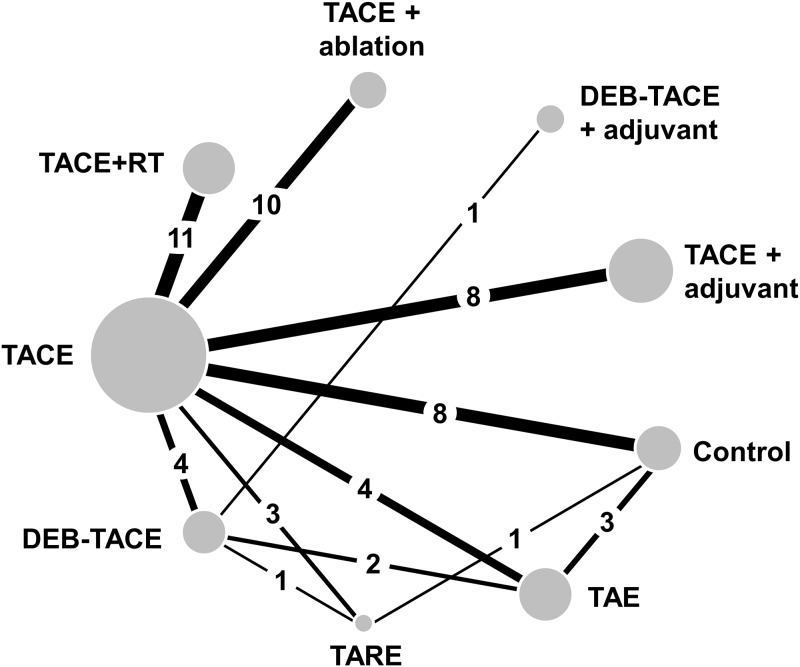
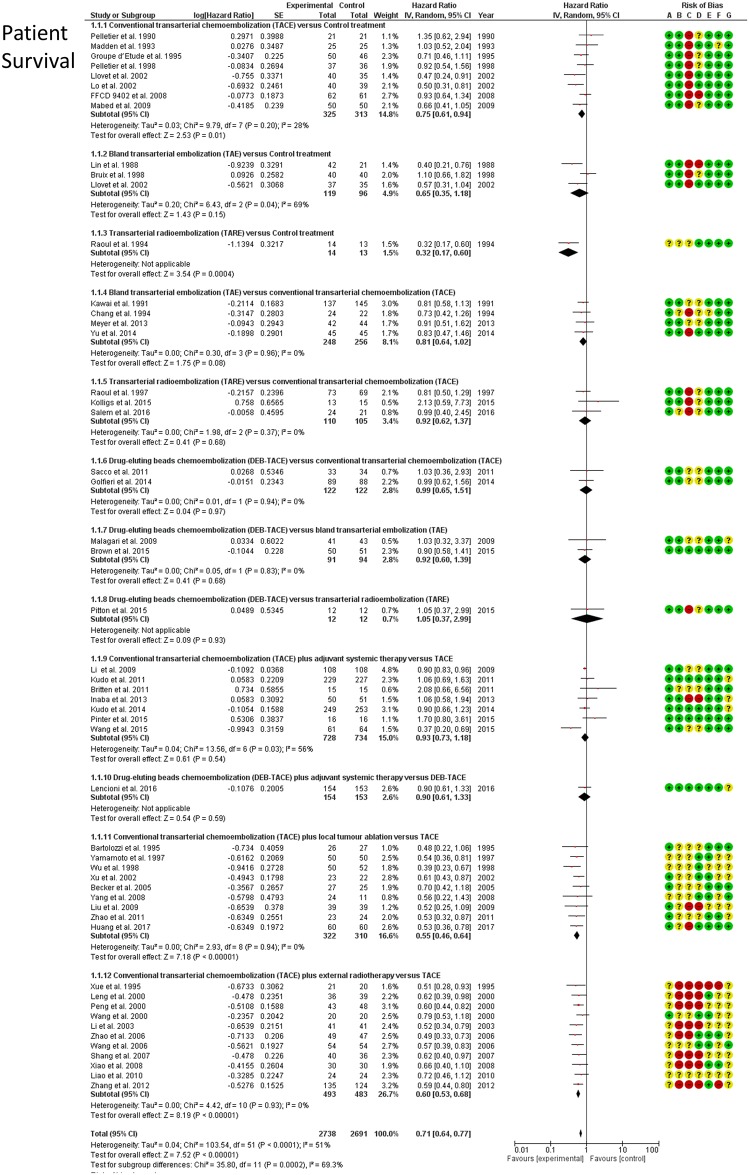
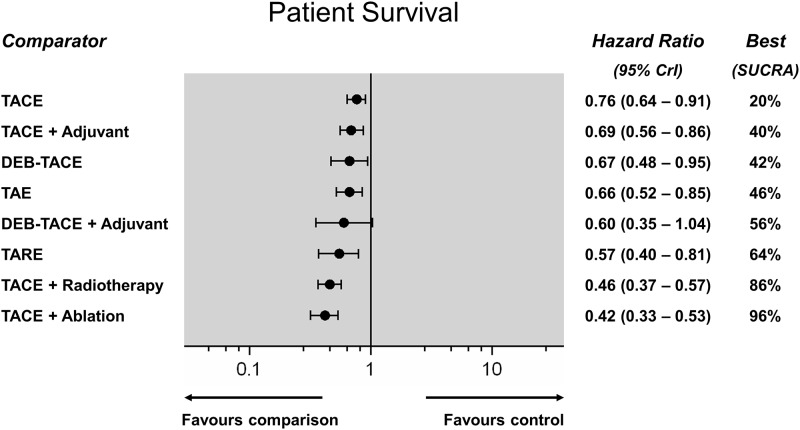
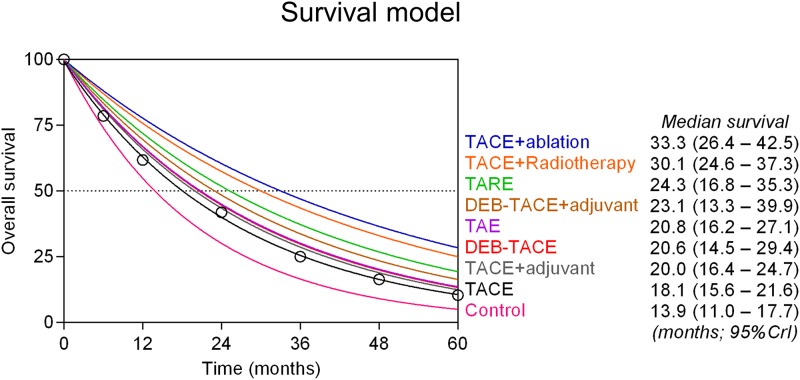
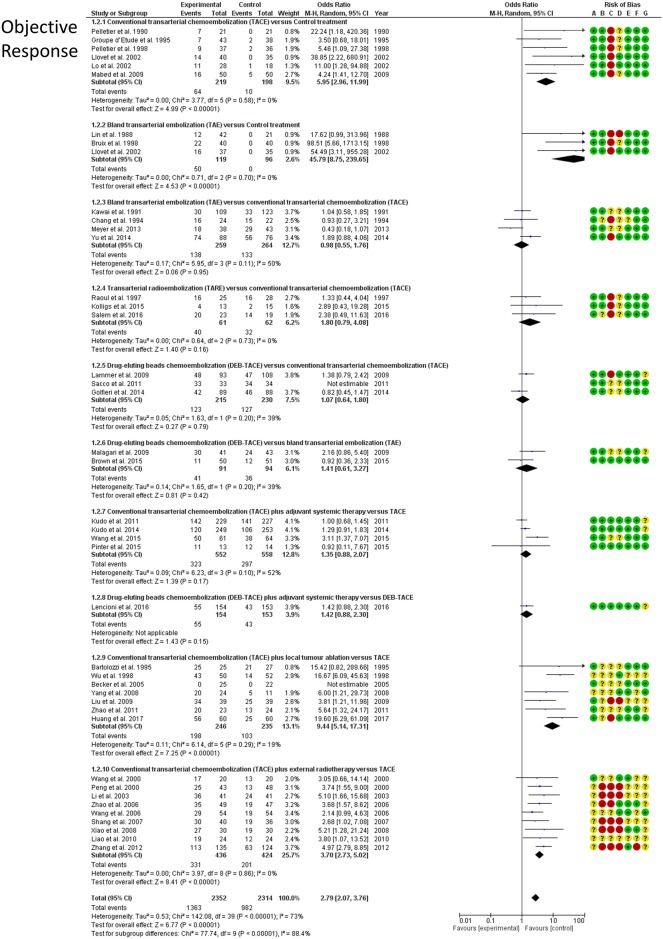
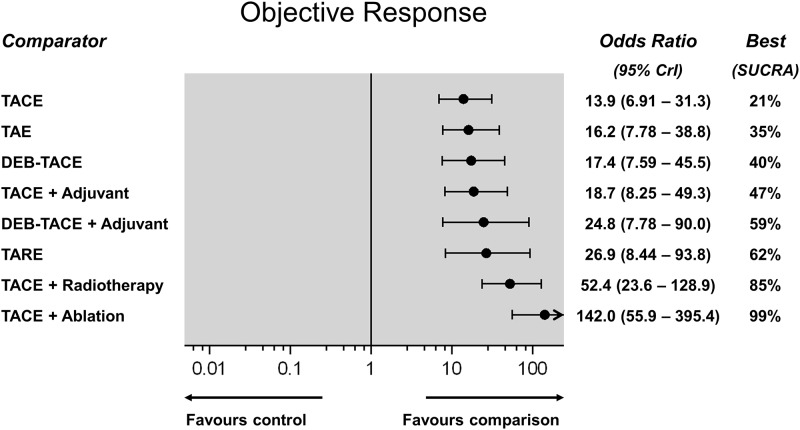
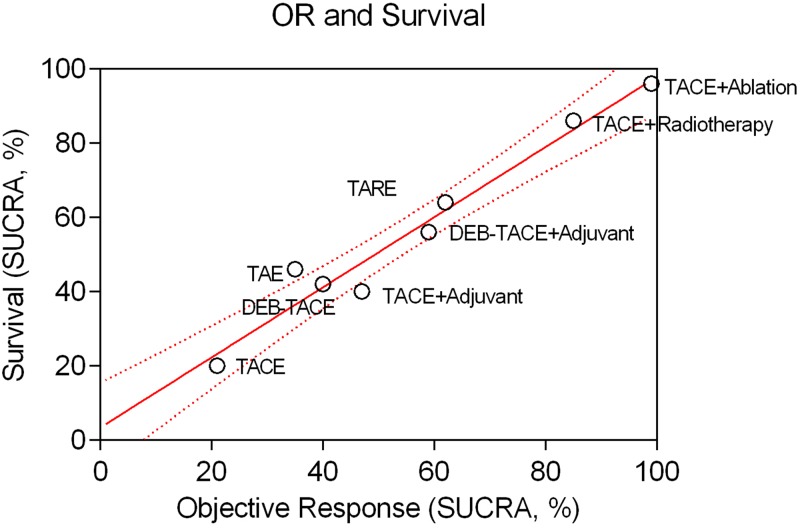
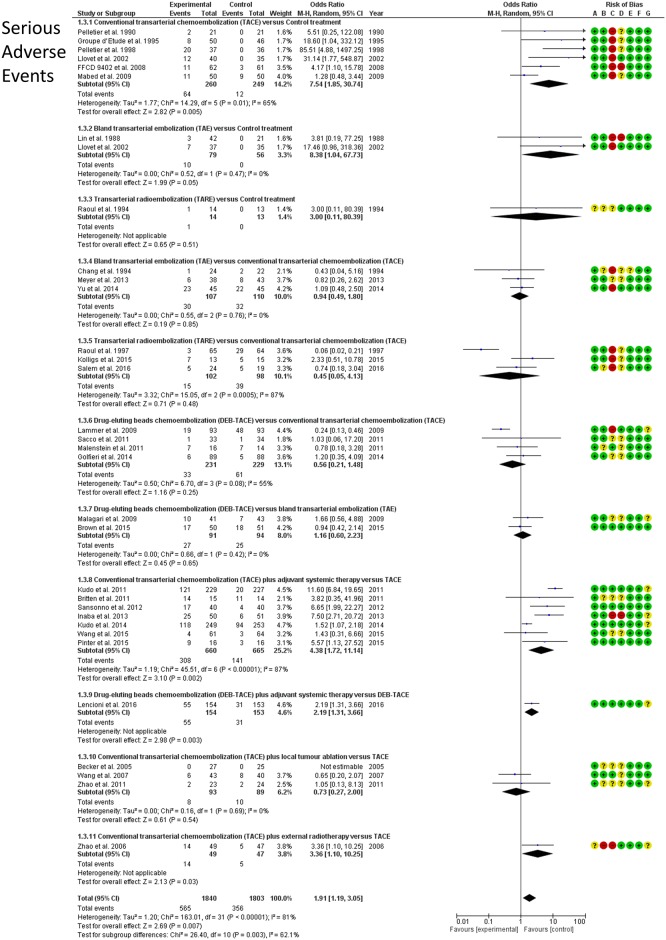
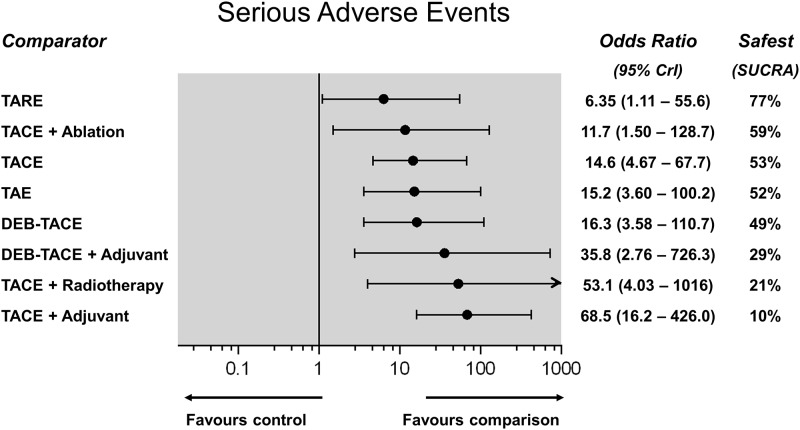
The network of evidence included 55 RCTs (12 direct comparisons) with 5,763 patients with preserved liver function and unresectable HCC (intermediate to advanced stage). All embolization strategies achieved a significant survival gain over control treatment (HR range, 0.42-0.76; very low-to-moderate QoE). However, TACE, DEB-TACE, TARE and adjuvant systemic agents did not confer any survival benefit over bland TAE alone (moderate QoE, except low in case of TARE). There was moderate QoE that TACE combined with external radiation or liver ablation achieved the best patient survival (SUCRA 86% and 96%, respectively). Estimated median survival was 13.9 months in control, 18.1 months in TACE, 20.6 months with DEB-TACE, 20.8 months with bland TAE, 30.1 months in TACE plus external radiotherapy, and 33.3 months in TACE plus liver ablation. TARE was the safest treatment (SUCRA 77%), however, all examined therapies were associated with a significantly higher risk of toxicity over control (OR range, 6.35 to 68.5). TACE, DEB-TACE, TARE and adjuvant systemic agents did not improve objective response over bland embolization alone (OR range, 0.85 to 1.65). There was clinical diversity among included randomized controlled trials, but statistical heterogeneity was low.
Chemo- and radio-embolization for unresectable hepatocellular carcinoma may improve tumour objective response and patient survival, but are not more effective than bland particle embolization. Chemoembolization combined with external radiotherapy or local liver ablation may significantly improve tumour response and patient survival rates over embolization monotherapies. Quality of evidence remains mostly low to moderate because of clinical diversity.
CRD42016035796 (http://www.crd.york.ac.uk/PROSPERO).
对于无法切除的肝细胞癌(HCC)患者,最佳的经导管栓塞策略仍不明确。我们对无法切除的HCC的不同栓塞方案进行了系统评价和网状Meta分析(NMA)。
检索医学数据库,查找截至2017年6月评估单纯性经动脉栓塞(TAE)、传统经动脉化疗栓塞(TACE)、载药微球化疗栓塞(DEB-TACE)或经动脉放射性栓塞(TARE),单独或联合辅助化疗、局部肝脏消融或外照射治疗无法切除的HCC的随机对照试验。采用具有二项式和正态似然性的随机效应贝叶斯模型(WinBUGS)进行拟合。主要终点是患者生存率,以风险比(HR)和95%可信区间表示。使用指数模型拟合患者生存曲线。安全性和客观缓解率计算为比值比(OR)及相应的95%可信区间。采用SUCRA统计量对相互竞争的治疗方法进行排序。计算异质性调整后的有效样本量,以评估每次比较的信息量。采用适用于NMA报告的GRADE系统评估证据质量(QoE)。所有分析均符合ISPOR-AMCP-NCP工作组关于NMA良好实践的报告。
证据网络包括55项随机对照试验(12项直接比较),共5763例肝功能良好且无法切除的HCC患者(中晚期)。与对照治疗相比,所有栓塞策略均显著提高了生存率(HR范围为0.42 - 0.76;证据质量从极低到中等)。然而,TACE、DEB-TACE、TARE和辅助全身治疗药物单独使用时,与单纯性TAE相比,并未带来任何生存获益(证据质量中等,TARE除外,其证据质量低)。有中等证据质量表明,TACE联合外照射或肝脏消融可使患者生存率最佳(SUCRA分别为86%和96%)。对照组的估计中位生存期为13.9个月,TACE组为18.1个月,DEB-TACE组为20.6个月,单纯性TAE组为20.8个月,TACE加外照射组为30.1个月,TACE加肝脏消融组为33.3个月。TARE是最安全的治疗方法(SUCRA为77%),然而,所有检查的治疗方法与对照相比,毒性风险均显著更高(OR范围为6.35至68.5)。TACE、DEB-TACE、TARE和辅助全身治疗药物单独使用时,与单纯性栓塞相比,并未改善客观缓解率(OR范围为0.85至1.65)。纳入的随机对照试验存在临床多样性,但统计异质性较低。
对于无法切除的肝细胞癌,化疗栓塞和放射性栓塞可能改善肿瘤客观缓解率和患者生存率,但并不比单纯性颗粒栓塞更有效。与栓塞单一疗法相比,化疗栓塞联合外照射或局部肝脏消融可能显著提高肿瘤缓解率和患者生存率。由于临床多样性,证据质量大多仍为低到中等。
CRD42016035796(http://www.crd.york.ac.uk/PROSPERO)