Warmerdam Mats, Stolwijk Frank, Boogert Anjelica, Sharma Meera, Tetteroo Lisa, Lucke Jacinta, Mooijaart Simon, Ansems Annemieke, Esteve Cuevas Laura, Rijpsma Douwe, de Groot Bas
Emergency Department, Leiden University Medical Centre, Leiden, Zuid-Holland, the Netherlands.
Department of Gerontology and Geriatrics, Leiden University Medical Centre, Leiden, Zuid-Holland, The Netherlands & Institute for Evidence-based Medicine in Old Age | IEMO, Leiden, The Netherlands.
PLoS One. 2017 Sep 25;12(9):e0185214. doi: 10.1371/journal.pone.0185214. eCollection 2017.
Due to atypical symptom presentation older patients are more prone to delayed sepsis recognition. We investigated whether initial disease severity before emergency department (ED) treatment (including treatable acute organ dysfunction), quality of ED sepsis care and the impact on mortality was different between patients older and younger than 70 years. If differences exist, improvements are needed for ED management of older patients at risk for sepsis.
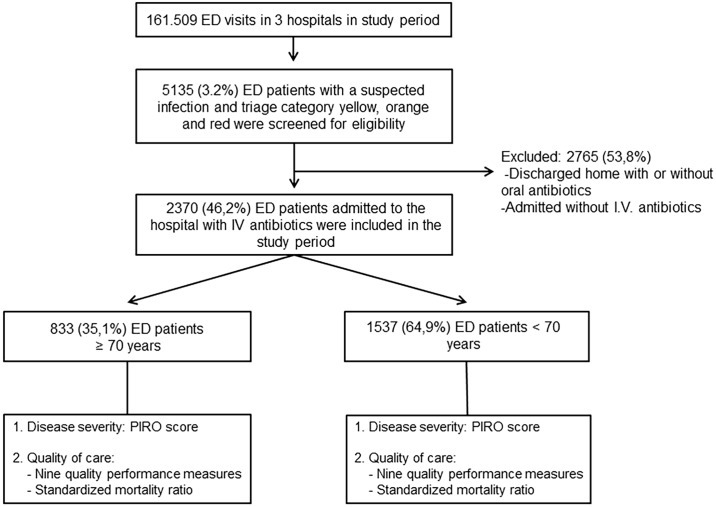
In this observational multicenter study, ED patients who were hospitalized with a suspected infection were stratified by age <70 and ≥70 years. The presence of treatable and potentially reversible acute organ dysfunction was measured by the RO components of the Predisposition, Infection, Response and Organ dysfunction (PIRO) score, reflecting acute sepsis-related organ dysfunction developed before ED presentation. Quality of care, as assessed by the full compliance with nine quality performance measures and the standardized mortality ratio (SMR: observed/expected in-hospital mortality), was compared between older and younger patients.
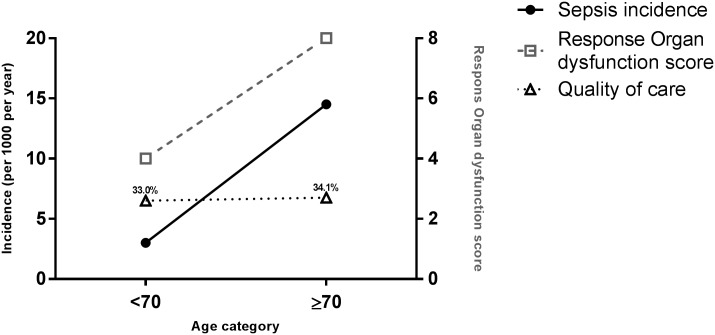
The RO-components of the PIRO score were 8 (interquartile range; 4-9) in the 833 older patients, twice as high as the 4 (2-8; P<0.001) in the 1537 younger patients. However, full compliance with all nine quality performance measures was achieved in 34.2 (31.0-37.4)% of the older patients, not higher than the 33.0 (30.7-35.4)% in younger patients (P = 0.640). In-hospital mortality was 9.2% (95%-CI, 7.3-11.2) in patients ≥70, twice as high as the 4.6% (3.6-5.6) in patients <70 years, resulting in an SMR (in study period) of ~0.7 in both groups (P>0.05).
Older sepsis patients are sicker at ED presentation but are not treated more expediently or reliably despite their extra acuity The presence of twice as much treatable acute organ dysfunction before ED treatment suggests that acute organ dysfunction is recognized relatively late by general practitioners or patients in the out of hospital setting.
由于症状表现不典型,老年患者更容易出现脓毒症识别延迟的情况。我们调查了70岁及以上和70岁以下患者在急诊科(ED)治疗前的初始疾病严重程度(包括可治疗的急性器官功能障碍)、ED脓毒症护理质量及其对死亡率的影响是否存在差异。如果存在差异,则需要改进对有脓毒症风险的老年患者的ED管理。
在这项观察性多中心研究中,因疑似感染而住院的ED患者按年龄<70岁和≥70岁进行分层。通过易感性、感染、反应和器官功能障碍(PIRO)评分的RO成分来衡量是否存在可治疗且可能可逆的急性器官功能障碍,该评分反映了在ED就诊前出现的急性脓毒症相关器官功能障碍。比较了老年患者和年轻患者在完全符合九项质量绩效指标方面的护理质量以及标准化死亡率(SMR:观察到的/预期的院内死亡率)。
833例老年患者PIRO评分的RO成分中位数为8(四分位间距;4 - 9),是1537例年轻患者(中位数为4,四分位间距为2 - 8;P<0.001)的两倍。然而,34.2(31.0 - 37.4)%的老年患者完全符合所有九项质量绩效指标,并不高于年轻患者中的33.0(30.7 - 35.4)%(P = 0.640)。70岁及以上患者的院内死亡率为9.2%(95%置信区间,7.3 - 11.2),是70岁以下患者4.6%(3.6 - 5.6)的两倍,两组的SMR(在研究期间)均约为0.7(P>0.05)。
老年脓毒症患者在ED就诊时病情更严重,但尽管他们病情更危急,却没有得到更迅速或可靠的治疗。在ED治疗前存在两倍多的可治疗急性器官功能障碍,这表明全科医生或患者在院外环境中对急性器官功能障碍的识别相对较晚。