Ferrandino Rocco, Roof Scott, Ma Yue, Chan Lili, Poojary Priti, Saha Aparna, Chauhan Kinsuk, Coca Steven G, Nadkarni Girish N, Teng Marita S
1 Icahn School of Medicine at Mount Sinai, New York, New York, USA.
2 Department of Otolaryngology-Head and Neck Surgery, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Otolaryngol Head Neck Surg. 2017 Dec;157(6):955-965. doi: 10.1177/0194599817721154. Epub 2017 Sep 26.
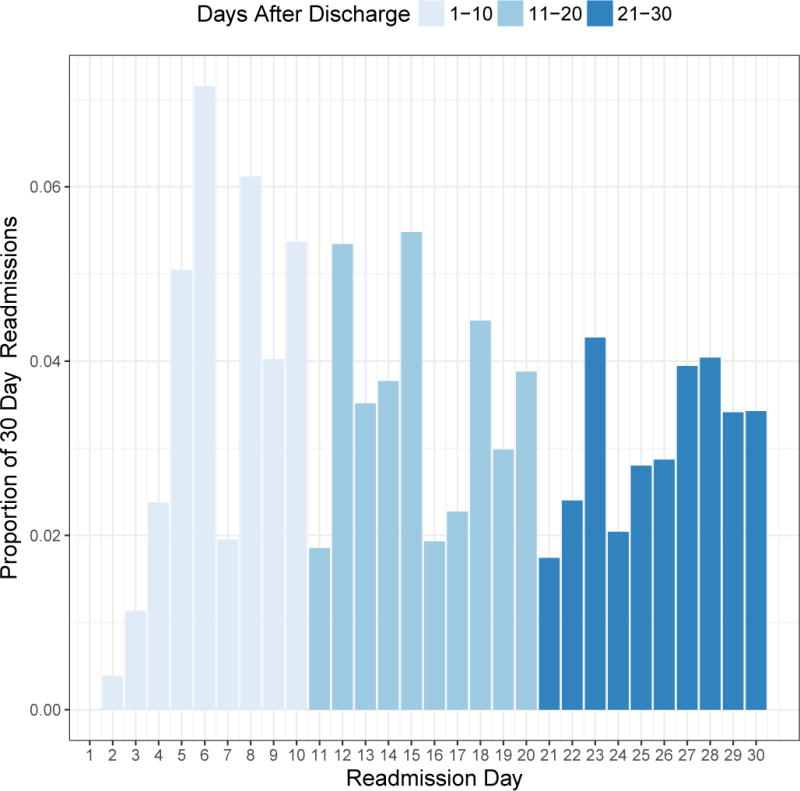
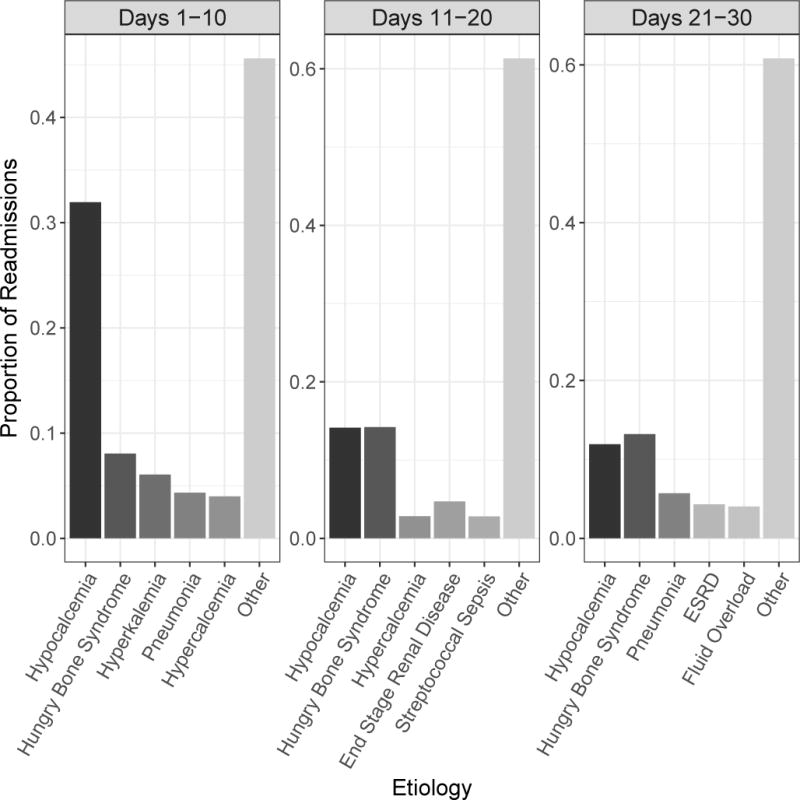
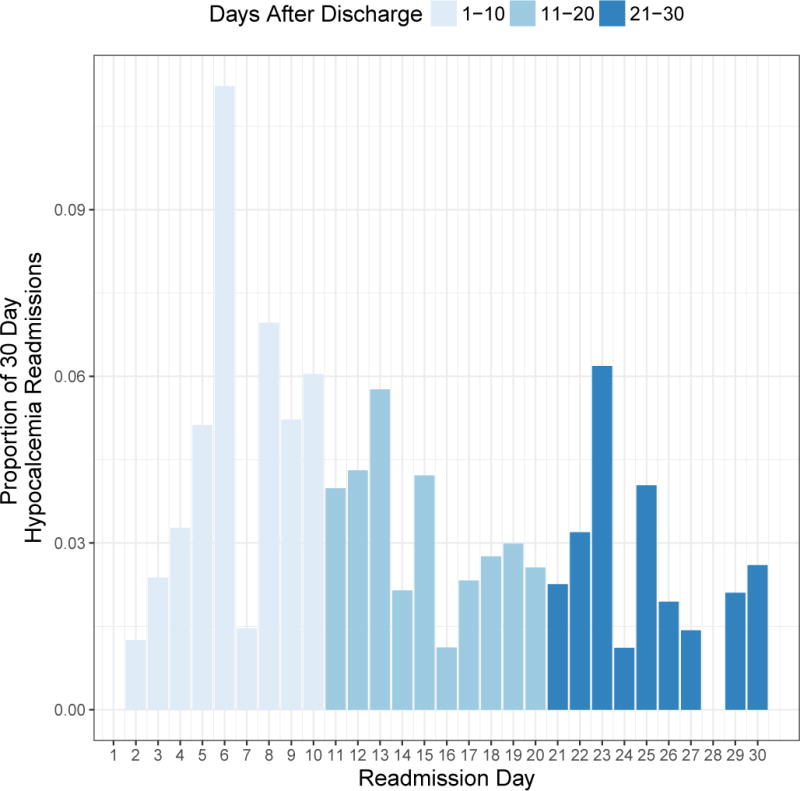
Objective To examine rates of readmission after parathyroidectomy in patients with chronic kidney disease and determine primary etiologies, timing, and risk factors for these unplanned readmissions. Study Design Retrospective cohort study. Setting Nationwide Readmissions Database. Subjects and Methods The Nationwide Readmissions Database was queried for parathyroidectomy procedures performed in patients with chronic kidney disease between January 2013 and November 2013. Patient-, admission-, and hospital-level characteristics were compared for patients with and without at least 1 unplanned 30-day readmission. Outcomes of interest included rates, etiology, and timing of readmission. Multivariate logistic regression was used to identify predictors of 30-day readmission. Results There were 2756 parathyroidectomies performed in patients with chronic kidney disease with an unplanned readmission rate of 17.2%. Hypocalcemia/hungry bone syndrome accounted for 40% of readmissions. Readmissions occurred uniformly throughout the 30 days after discharge, but readmissions for hypocalcemia/hungry bone syndrome peaked in the first 10 days and decreased over time. Weight loss/malnutrition at time of parathyroidectomy and length of stay of 5 to 6 days conferred increased risk of readmission with adjusted odds ratios (aOR) of 3.31 (95% confidence interval [CI], 1.55-7.05; P = .002) and 1.87 (95% CI, 1.10-3.19; P = .02), respectively. Relative to primary hyperparathyroidism, parathyroidectomies performed for secondary hyperparathyroidism (aOR, 2.53; 95% CI, 1.07-5.95; P = .03) were associated with higher risk of readmission. Conclusion Postparathyroidectomy readmission rates for patients with chronic kidney disease are nearly 5 times that of the general population. Careful consideration of postoperative care and electrolyte management is crucial to minimize preventable readmissions in this vulnerable population.
目的 研究慢性肾病患者甲状旁腺切除术后的再入院率,确定这些非计划再入院的主要病因、时间及风险因素。研究设计 回顾性队列研究。研究地点 全国再入院数据库。研究对象与方法 查询全国再入院数据库中2013年1月至2013年11月期间慢性肾病患者接受甲状旁腺切除术的情况。比较有至少1次非计划30天再入院和无再入院患者的患者、入院及医院层面特征。关注的结局包括再入院率、病因及时间。采用多因素逻辑回归确定30天再入院的预测因素。结果 慢性肾病患者共进行了2756例甲状旁腺切除术,非计划再入院率为17.2%。低钙血症/饥饿骨综合征占再入院原因的40%。出院后30天内再入院情况均匀分布,但低钙血症/饥饿骨综合征导致的再入院在术后前10天达到高峰并随时间下降。甲状旁腺切除时体重减轻/营养不良以及住院时间为5至6天会增加再入院风险,校正优势比(aOR)分别为3.31(95%置信区间[CI],1.55 - 7.05;P = 0.002)和1.87(95% CI,1.10 - 3.19;P = 0.02)。相对于原发性甲状旁腺功能亢进,因继发性甲状旁腺功能亢进进行的甲状旁腺切除术(aOR,2.53;95% CI,1.07 - 5.95;P = 0.03)与更高的再入院风险相关。结论 慢性肾病患者甲状旁腺切除术后再入院率几乎是普通人群的5倍。仔细考虑术后护理和电解质管理对于减少这一脆弱人群中可预防的再入院至关重要。