Briones Melissa R, Morgan Gabrielle A, Amoruso Maria C, Rahmani Bahram, Ryan Maura E, Pachman Lauren M
Division of Allergy, Immunology, and Rheumatology, Loyola University Medical Center, Maywood, USA.
Pediatrics, Stanly Manne Children's Research Institute, Children's Hospital of Chicago; Ann and Robert H. Lurie Children's Hospital, Chicago, USA.
RMD Open. 2017 Jul 11;3(1):e000385. doi: 10.1136/rmdopen-2016-000385. eCollection 2017.
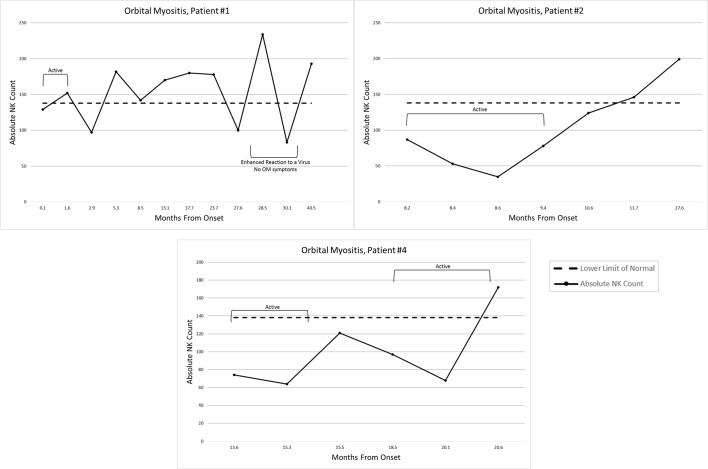
The study aimed to document the utility of the absolute number of natural killer cells as a biomarker in paediatric orbital myositis (OM). Extracted data from four children with OM included demographics, laboratory values, imaging and treatment response. Stored sera (-80°C) were tested for IgG4 levels in three cases and antibody to Coxsackie B in two cases. Their first symptom was at 14.4±1.2 years (mean±SD). At diagnosis three had creatine phosphokinase (CPK) of 97.3±44.2, aldolase of 8.5±2.8 (n=2), alanine aminotransferase (ALT) of 13±2.8 (n=2) and aspartate aminotransferase (AST) of 21.3±2.9. IG4 level was 87.7±66 (normal=8-89 mg/dL); two sera (patients 1and4) were positive (>1:8 dilution) for anti-Coxsackievirus antigen B5. The CD3-CD16+CD56+ natural killer absolute count was 96.7±28.7 (lower limit of normal=138), increasing to 163±57.2 with disease resolution in three patients. The fourth patient was followed elsewhere. CT showed involvement of bilateral superior oblique, lateral rectus or the left medial rectus muscles. Treatment included intravenous methylprednisolone, methotrexate (n=2) and other immunosuppressants. Paediatric OM disease activity was associated with initially low absolute CD3-CD16+CD56+ natural killer cell counts, which normalised with improvement. We speculate (1) infection, such as Coxsackie B virus, may be associated with paediatric OM; and (2) the absolute count of circulating CD3-CD16+CD56+ natural killer lymphocytes may serve as a biomarker to guide medical therapy.
该研究旨在记录自然杀伤细胞绝对数量作为小儿眼眶肌炎(OM)生物标志物的效用。从4例OM患儿中提取的数据包括人口统计学信息、实验室检查值、影像学检查及治疗反应。3例患儿的储存血清(-80°C)检测了IgG4水平,2例检测了抗柯萨奇B抗体。他们的首发症状出现在14.4±1.2岁(均值±标准差)。诊断时,3例患儿的肌酸磷酸激酶(CPK)为97.3±44.2,醛缩酶为8.5±2.8(n=2),丙氨酸氨基转移酶(ALT)为13±2.8(n=2),天冬氨酸氨基转移酶(AST)为21.3±2.9。IgG4水平为87.7±66(正常范围=8-89mg/dL);2份血清(患者1和4)抗柯萨奇病毒抗原B5呈阳性(>1:8稀释度)。CD3-CD16+CD56+自然杀伤细胞绝对计数为96.7±28.7(正常下限=138),3例患者病情缓解后增至163±57.2。第4例患者在其他地方接受随访。CT显示双侧上斜肌、外直肌或左侧内直肌受累。治疗包括静脉注射甲泼尼龙、甲氨蝶呤(n=2)及其他免疫抑制剂。小儿OM疾病活动与最初较低的CD3-CD16+CD56+自然杀伤细胞绝对计数相关,病情改善时该计数恢复正常。我们推测:(1)感染,如柯萨奇B病毒,可能与小儿OM有关;(2)循环CD3-CD16+CD56+自然杀伤淋巴细胞的绝对计数可作为指导药物治疗的生物标志物。