Bilinski Alyssa, Birru Ermyas, Peckarsky Matthew, Herce Michael, Kalanga Noel, Neumann Christian, Bronson Gay, Po-Chedley Stephen, Kachimanga Chembe, McBain Ryan, Keck James
Abwenzi Pa Za Umoyo, Neno, Malawi and Partners In Health, Boston, Massachusetts, United States of America.
Interfaculty Initiative in Health Policy, Harvard Graduate School of Arts and Sciences, Cambridge, Massachusetts, United States of America.
PLoS One. 2017 Oct 3;12(10):e0185699. doi: 10.1371/journal.pone.0185699. eCollection 2017.
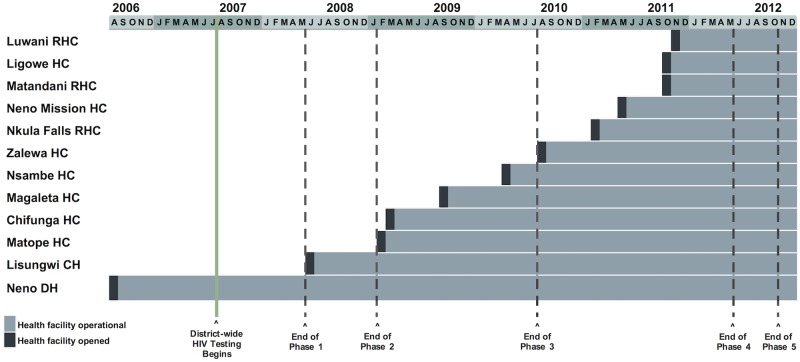
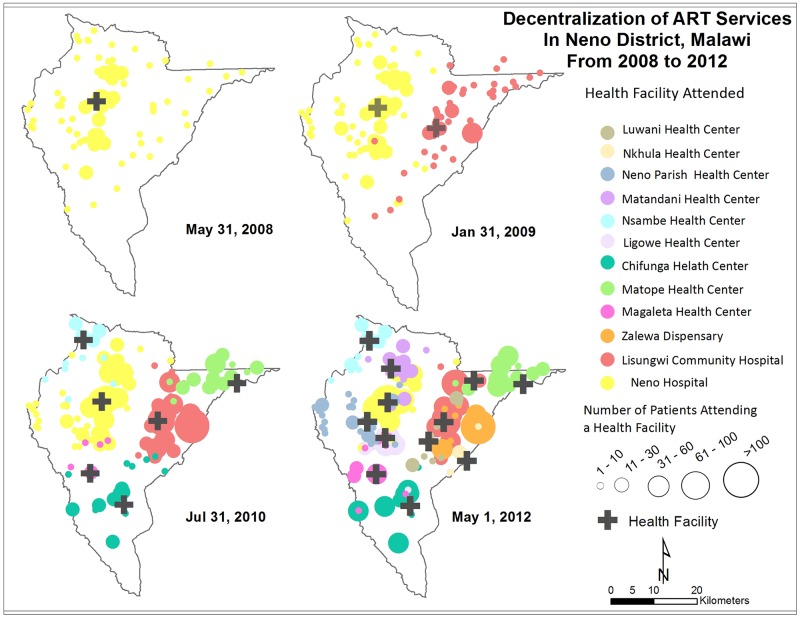
HIV/AIDS remains the second most common cause of death in low and middle-income countries (LMICs), and only 34% of eligible patients in Africa received antiretroviral therapy (ART) in 2013. This study investigated the impact of ART decentralization on patient enrollment and retention in rural Malawi. We reviewed electronic medical records of patients registered in the Neno District ART program from August 1, 2006, when ART first became available, through December 31, 2013. We used GPS data to calculate patient-level distance to care, and examined number of annual ART visits and one-year lost to follow-up (LTFU) in HIV care. The number of ART patients in Neno increased from 48 to 3,949 over the decentralization period. Mean travel distance decreased from 7.3 km when ART was only available at the district hospital to 4.7 km when ART was decentralized to 12 primary health facilities. For patients who transferred from centralized care to nearer health facilities, mean travel distance decreased from 9.5 km to 4.7 km. Following a transfer, the proportion of patients achieving the clinic's recommended ≥4 annual visits increased from 89% to 99%. In Cox proportional hazards regression, patients living ≥8 km from a health facility had a greater hazard of being LTFU compared to patients <8 km from a facility (adjusted HR: 1.7; 95% CI: 1.5-1.9). ART decentralization in Neno District was associated with increased ART enrollment, decreased travel distance, and increased retention in care. Increasing access to ART by reducing travel distance is one strategy to achieve the ART coverage and viral suppression objectives of the 90-90-90 UNAIDS targets in rural impoverished areas.
艾滋病毒/艾滋病仍是低收入和中等收入国家(LMICs)第二大常见死因,2013年非洲仅有34%符合条件的患者接受了抗逆转录病毒疗法(ART)。本研究调查了抗逆转录病毒疗法去中心化对马拉维农村地区患者登记和留存率的影响。我们回顾了从2006年8月1日(抗逆转录病毒疗法首次可用)至2013年12月31日在尼昂区抗逆转录病毒疗法项目中登记的患者的电子病历。我们使用全球定位系统(GPS)数据计算患者到医疗机构的距离,并检查了艾滋病毒护理中每年抗逆转录病毒疗法就诊次数和失访一年(LTFU)的情况。在去中心化期间,尼昂区接受抗逆转录病毒疗法的患者人数从48人增加到3949人。平均出行距离从仅在区医院提供抗逆转录病毒疗法时的7.3公里降至抗逆转录病毒疗法去中心化至12个初级卫生设施时的4.7公里。对于从集中护理转移到更近医疗机构的患者,平均出行距离从9.5公里降至4.7公里。转移后,达到诊所建议的每年≥4次就诊的患者比例从89%增至99%。在Cox比例风险回归中,与距离医疗机构<8公里的患者相比,距离医疗机构≥8公里的患者失访风险更高(调整后风险比:1.7;95%置信区间:1.5 - 1.9)。尼昂区的抗逆转录病毒疗法去中心化与抗逆转录病毒疗法登记人数增加、出行距离缩短以及护理留存率提高相关。通过缩短出行距离增加获得抗逆转录病毒疗法的机会是在农村贫困地区实现联合国艾滋病规划署90 - 90 - 90目标中抗逆转录病毒疗法覆盖和病毒抑制目标的一项策略。