LAC+USC Medical Center, Keck School of Medicine, Los Angeles, CA, USA.
Coordinating Center for Clinical Trials, University of Texas School of Public Health, Houston, TX, USA.
J Natl Med Assoc. 2017;109(3):172-181. doi: 10.1016/j.jnma.2017.02.005. Epub 2017 Mar 18.
Limited information is available on long-term antihypertensive and lipid-lowering therapy effects on hypertensive patients with atrial fibrillation/flutter (AF/AFL) compared to those without. AF/AFL at baseline or during the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) (mean follow-up 4.9 years) markedly increased risk of stroke, heart failure, CHD, and all-cause mortality. We aimed to determine if AF/AFL continued to impact outcomes during post-trial follow-up (mean 3.8 years).
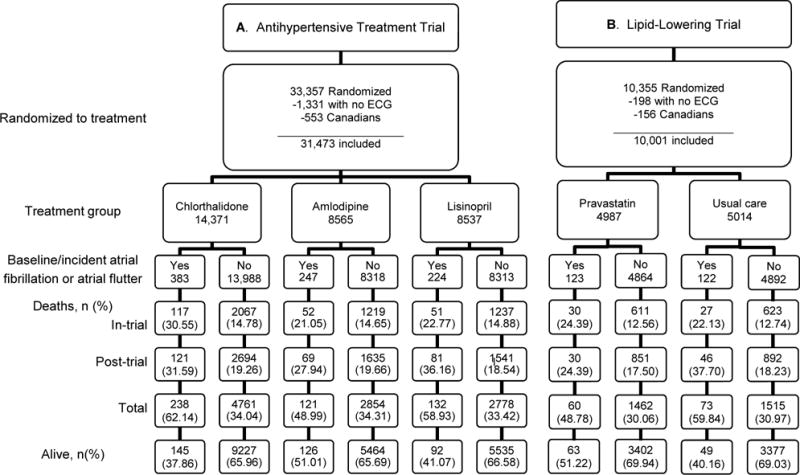
Patients were randomized to chlorthalidone, amlodipine, or lisinopril, and to pravastatin vs. usual care in the lipid-lowering trial (LLT). Of 31,473 available subjects, AF/AFL occurred in 854; 383/14,371 chlorthalidone (2.7%), 247/8565 amlodipine (2.9%), and 224/8537 lisinopril (2.6%). Post-hoc analyses utilized administrative databases for post-trial data. Individuals with AF/AFL were compared to those without during post-trial. Outcomes were analyzed by treatment groups for the antihypertensive and LLT trials.
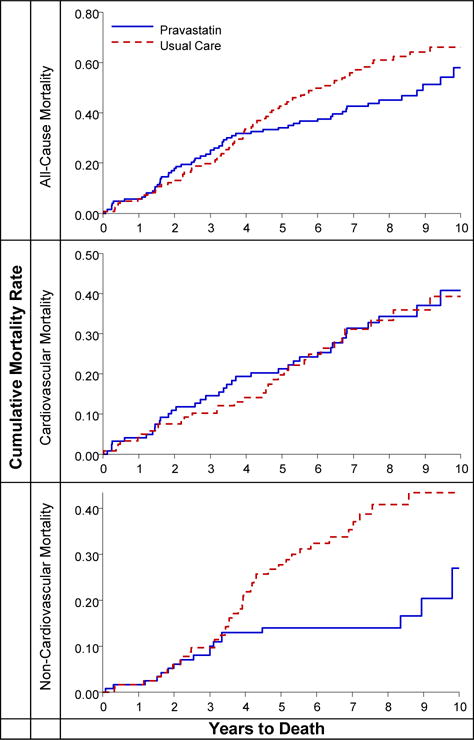
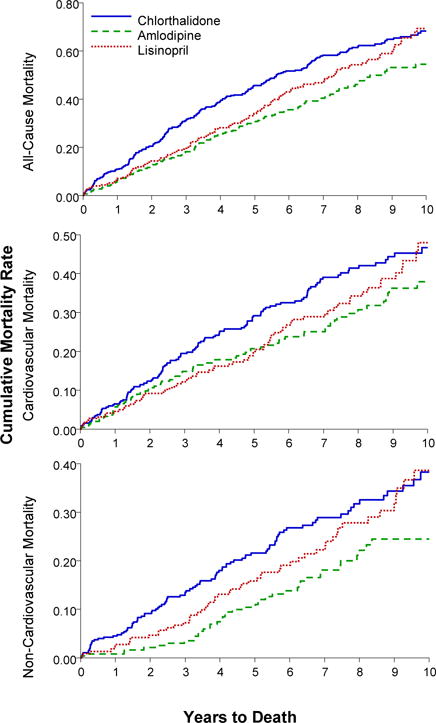
Among 854 AF/AFL participants, 491 (57.5%) died: 220 in-trial, 271 post-trial. Ten-year all-cause mortality rates for those with in-trial AF/AFL were similar for chlorthalidone and lisinopril, but lower for amlodipine (68, 66, and 49 per 100 persons, respectively); adjusted HR for amlodipine vs. chlorthalidone was 0.68 (95% CI, 0.54-0.87). Ten-year all-cause mortality rates were 57 vs. 65 per 100 persons (pravastatin vs. usual care); non-CVD mortality rates, 18 vs. 39 per 100 persons (pravastatin vs. usual care) (adjusted HR = 0.46, 95% CI, 0.24-0.86).
Post-trial follow-up revealed continued deleterious AF/AFL effects. The amlodipine (ALLHAT) and pravastatin (ALLHAT-LLT) treatment groups showed lower all-cause and non-CVD mortality compared to the chlorthalidone and usual-care groups, respectively.
与无房颤/房扑(AF/AFL)的高血压患者相比,关于长期降压和降脂治疗对 AF/AFL 患者的影响,目前仅有有限的信息。在高血压和降脂治疗预防心脏病试验(ALLHAT)中,基线时或试验期间存在 AF/AFL(平均随访 4.9 年)明显增加了中风、心力衰竭、冠心病和全因死亡率的风险。我们旨在确定 AF/AFL 在试验后随访期间(平均 3.8 年)是否仍会影响结局。
患者被随机分配至氯噻酮、氨氯地平或赖诺普利,并在降脂试验(LLT)中接受普伐他汀或常规治疗。在 31473 名可评估的受试者中,854 名发生了 AF/AFL;氯噻酮组 383/14371(2.7%)、氨氯地平组 247/8565(2.9%)和赖诺普利组 224/8537(2.6%)。利用事后分析获取试验后数据的行政数据库。在试验后,将有 AF/AFL 的个体与无 AF/AFL 的个体进行比较。分析按降压和降脂试验的治疗组进行结局。
在 854 名 AF/AFL 参与者中,491 人(57.5%)死亡:220 人在试验中死亡,271 人在试验后死亡。有 AF/AFL 的患者在试验期间的 10 年全因死亡率在氯噻酮和赖诺普利组之间相似,但在氨氯地平组中较低(分别为 68、66 和 49 每 100 人);与氯噻酮相比,氨氯地平的调整后的 HR 为 0.68(95%CI,0.54-0.87)。10 年全因死亡率分别为 57 比 65 每 100 人(普伐他汀比常规治疗);非心血管死亡率分别为 18 比 39 每 100 人(普伐他汀比常规治疗)(调整后的 HR=0.46,95%CI,0.24-0.86)。
试验后随访显示持续存在的 AF/AFL 有害影响。与氯噻酮和常规治疗组相比,氨氯地平(ALLHAT)和普伐他汀(ALLHAT-LLT)治疗组的全因和非心血管死亡率均较低。