Park Seong Jun, Kwon Chang Hee, Bae Byeong Joo, Kim Bum Sung, Kim Sung Hea, Kim Hyun-Joong, Hwang Hweung Kon, Chung Sang-Man
The Department of Internal Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
Medicine (Baltimore). 2017 Oct;96(43):e8430. doi: 10.1097/MD.0000000000008430.
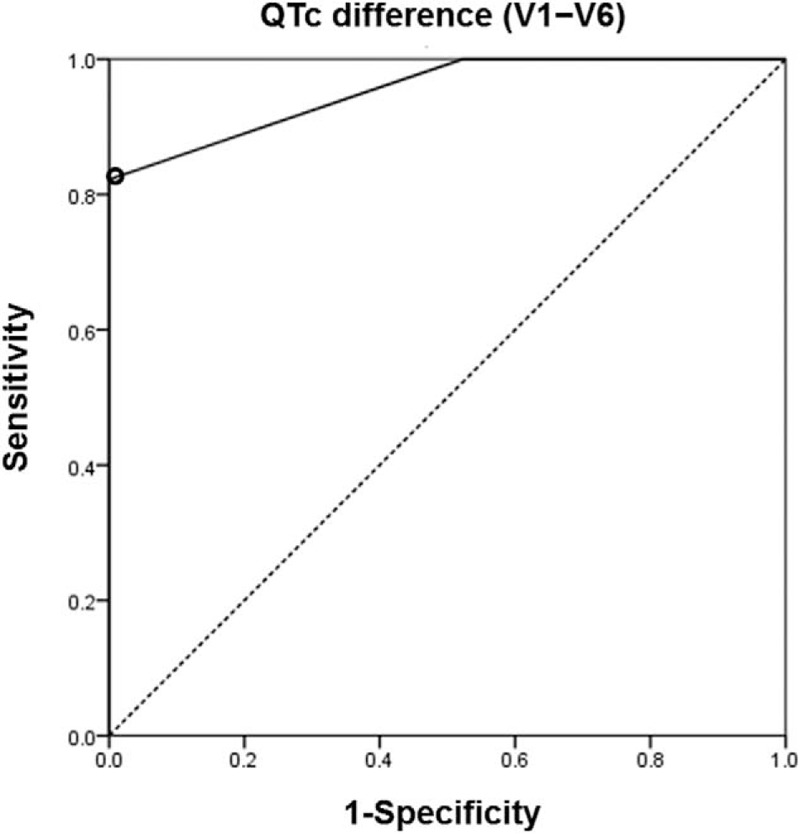
In acute pulmonary thromboembolism (PTE), right ventricular pressure overload impairs right-sided cardiac conduction and repolarization. We hypothesized that if heterogeneity of repolarization between right and left ventricles occurs in acute PTE, there would be the difference of repolarization between them. Therefore, we aimed to evaluate the diagnostic value of corrected QT interval (QTc) difference between leads V1 and V6 (V1 - V6) in patients with acute PTE.A total of 89 patients with suspected acute PTE who underwent computed tomographic angiography (CTA) were enrolled from January to December 2015. PTE was identified by CTA. We compared electrocardiographic (ECG) parameters, especially QTc difference (V1 - V6) between patients with PTE and those without PTE.Acute PTE was finally diagnosed in 45 patients. Clinical situations including the chief complaint were not different between PTE and non-PTE groups. S1Q3T3, a traditional ECG marker, had no diagnostic value for acute PTE. Patients with PTE had a significantly longer mean QTc in V1 (454.6 ± 44.3 vs 417.5 ± 31.3 ms, P < .001) and larger QTc difference (V1 - V6) (34.8 ± 30.5 vs -12.5 ± 16.6 ms, P < .001) than non-PTE controls. QTc difference (V1 - V6) was negative in all patients without PTE. PTE patients had a higher prevalence of T wave inversion in leads III (51.1% vs 29.5%, P = .038) and V1 (82.2% vs 38.6%, P < .001). A QTc difference (V1 - V6) of ≥20 ms identified PTE with 82.2% sensitivity, 100.0% specificity, and 100.0% positive predictive value.QTc difference (V1 - V6) had an excellent diagnostic value for differentiating patients with and without acute PTE.
在急性肺血栓栓塞症(PTE)中,右心室压力过载会损害右侧心脏传导和复极化。我们假设,如果急性PTE患者左右心室之间存在复极化异质性,那么它们之间会存在复极化差异。因此,我们旨在评估V1和V6导联(V1-V6)校正QT间期(QTc)差异对急性PTE患者的诊断价值。
2015年1月至12月,共纳入89例疑似急性PTE且接受计算机断层血管造影(CTA)检查的患者。通过CTA确诊PTE。我们比较了PTE患者和非PTE患者的心电图(ECG)参数,尤其是QTc差异(V1-V6)。
最终确诊45例急性PTE患者。PTE组和非PTE组的临床情况(包括主要症状)无差异。传统心电图标志物S1Q3T3对急性PTE无诊断价值。与非PTE对照组相比,PTE患者V1导联的平均QTc显著更长(454.6±44.3 vs 417.5±31.3毫秒,P<.001),QTc差异(V1-V6)更大(34.8±30.5 vs -12.5±16.6毫秒,P<.001)。所有非PTE患者的QTc差异(V1-V6)均为阴性。PTE患者III导联(51.1% vs 29.5%,P=.038)和V1导联(82.2% vs 38.6%,P<.001)T波倒置的发生率更高。QTc差异(V1-V6)≥20毫秒诊断PTE的敏感度为82.2%,特异度为100.0%,阳性预测值为100.0%。
QTc差异(V1-V6)对鉴别急性PTE患者和非急性PTE患者具有优异的诊断价值。