Department of Surgery, Chang Gung Memorial Hospital, No. 5, Fuxing St., Guishan Dist., Taoyuan, 333, Taiwan, Republic of China.
College of Medicine, Chang Gung University, Taoyuan, Taiwan, Republic of China.
BMC Cancer. 2017 Nov 9;17(1):742. doi: 10.1186/s12885-017-3748-9.
Liver resection had been regarded as a standard treatment for primary hepatocellular carcinoma (HCC). However, early mortality and recurrence after surgery were still of major concern. RAM (Risk Assessment for early Mortality) scoring system is a newly developed tool for assessing early mortality after hepatectomy for HCC. In this study, we compared RAM scoring system with ALBI and MELD scores for their capability of predicting short-term outcome.
We retrospectively reviewed patients with hepatocellular carcinoma who were treated with hepatectomy at Chang Gung Memorial Hospital between 1986 and 2015. Their clinical characteristics and perioperative variables were collected. We applied RAM, albumin-bilirubin (ALBI), and model for end-stage liver disease (MELD) scoring systems to predict early mortality and early recurrence in HCC patients after surgery. We investigated the discriminative power of each scoring system by receiver operating characteristic (ROC) curve and area under the ROC curve (AUC).
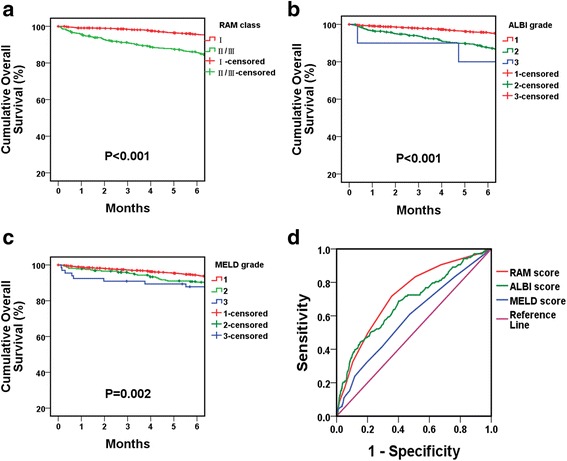
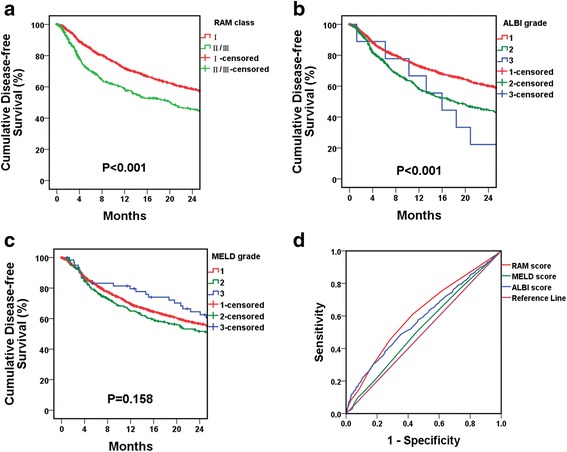
A total of 1935 patients (78% male) who underwent liver resection for HCC were included in this study. The median follow-up period was 41.9 months. One hundred and forty-nine patients (7.7%) died within 6 months after hepatectomy (early mortality). All the three scoring systems were effective predictor for early mortality, with higher score indicating higher risk of early mortality (AUC of RAM = 0.723, p < 0.001; AUC of ALBI = 0.682, p < 0.001; AUC of MELD = 0.590, p = 0.002). Cox regression multivariate analysis demonstrated that the RAM class was the most significant independent predictor of early mortality after surgery, while MELD grade failed to discriminatively predict early mortality. In addition to early mortality, the RAM score was also predictive of early recurrence in HCC after surgery.
This study demonstrated that RAM score is an effective and user-friendly bedside scoring system to predict early mortality and early recurrence after hepatectomy for HCC. In addition, the predictive capability of RAM score is superior to ALBI and MELD scores. Further study is warranted to validate our findings.
肝切除术一直被认为是原发性肝细胞癌 (HCC) 的标准治疗方法。然而,手术后的早期死亡率和复发仍然是主要关注点。RAM(早期死亡率风险评估)评分系统是一种新开发的用于评估 HCC 肝切除术后早期死亡率的工具。在本研究中,我们比较了 RAM 评分系统与 ALBI 和 MELD 评分系统在预测短期预后方面的能力。
我们回顾性分析了 1986 年至 2015 年期间在长庚纪念医院接受肝切除术治疗的 HCC 患者。收集了他们的临床特征和围手术期变量。我们应用 RAM、白蛋白-胆红素 (ALBI) 和终末期肝病模型 (MELD) 评分系统预测 HCC 患者手术后的早期死亡率和早期复发。我们通过接收者操作特征 (ROC) 曲线和 ROC 曲线下面积 (AUC) 来研究每个评分系统的判别能力。
共纳入 1935 例 (78%为男性) 接受 HCC 肝切除术的患者。中位随访时间为 41.9 个月。149 例患者 (7.7%) 在肝切除术后 6 个月内死亡 (早期死亡率)。所有三种评分系统均为早期死亡率的有效预测指标,评分越高,早期死亡率的风险越高 (RAM 评分的 AUC = 0.723,p < 0.001;ALBI 评分的 AUC = 0.682,p < 0.001;MELD 评分的 AUC = 0.590,p = 0.002)。Cox 回归多变量分析表明,RAM 分级是手术后早期死亡率的最显著独立预测因素,而 MELD 分级无法区分地预测早期死亡率。除了早期死亡率,RAM 评分还可预测 HCC 手术后的早期复发。
本研究表明,RAM 评分是一种有效且易于使用的床边评分系统,可预测 HCC 肝切除术后的早期死亡率和早期复发。此外,RAM 评分的预测能力优于 ALBI 和 MELD 评分。需要进一步的研究来验证我们的发现。