Scientific Institute for Quality of Healthcare, Celsus Academy for Sustainable Healthcare, Radboud university medical center, Nijmegen, The Netherlands.
Kenniscentrum - Research Consultancy, Zilveren Kruis, Zwolle, The Netherlands.
BMJ Open. 2017 Nov 12;7(11):e017775. doi: 10.1136/bmjopen-2017-017775.
To determine medical needs, demographic characteristics and healthcare utilisation patterns of the top 1% and top 2%-5% high-cost beneficiaries in the Netherlands.
Cross-sectional study using 1 year claims data. We broke down high-cost beneficiaries by demographics, the most cost-incurring condition per beneficiary and expensive treatment use.
Dutch curative health system, a health system with universal coverage.
4.5 million beneficiaries of one health insurer.
Annual total costs through hospital, intensive care unit use, expensive drugs, other pharmaceuticals, mental care and others; demographics; most cost-incurring and secondary conditions; inpatient stay; number of morbidities; costs per ICD10-chapter (International Statistical Classification of Diseases, 10th revision); and expensive treatment use (including dialysis, transplant surgery, expensive drugs, intensive care unit and diagnosis-related groups >€30 000).
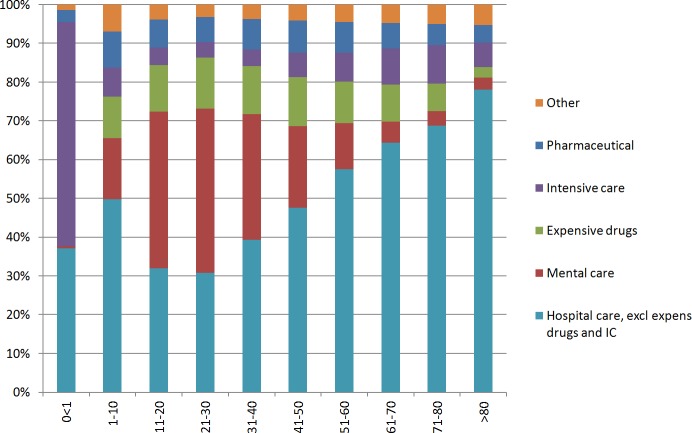
The top 1% and top 2%-5% beneficiaries accounted for 23% and 26% of total expenditures, respectively. Among top 1% beneficiaries, hospital care represented 76% of spending, of which, respectively, 9.0% and 9.1% were spent on expensive drugs and ICU care. We found that 54% of top 1% beneficiaries were aged 65 years or younger and that average costs sharply decreased with higher age within the top 1% group. Expensive treatments contributed to high costs in one-third of top 1% beneficiaries and in less than 10% of top 2%-5% beneficiaries. The average number of conditions was 5.5 and 4.0 for top 1% and top 2%-5% beneficiaries, respectively. 53% of top 1% beneficiaries were treated for circulatory disorders but for only 22% of top 1% beneficiaries this was their most cost-incurring condition.
Expensive treatments, most cost-incurring condition and age proved to be informative variables for studying this heterogeneous population. Expensive treatments play a substantial role in high-costs beneficiaries. Interventions need to be aimed at beneficiaries of all ages; a sole focus on the elderly would leave many high-cost beneficiaries unaddressed. Tailored interventions are needed to meet the needs of high-cost beneficiaries and to avoid waste of scarce resources.
确定荷兰前 1%和前 2%-5%高费用受益人的医疗需求、人口统计学特征和医疗保健利用模式。
使用 1 年索赔数据的横断面研究。我们根据人口统计学特征、每位受益人的最昂贵费用疾病和昂贵治疗的使用情况对高费用受益人进行细分。
荷兰治疗保健系统,一种具有全民覆盖的保健系统。
一家健康保险公司的 450 万受益人。
通过医院、重症监护病房使用、昂贵药物、其他药物、精神保健和其他方面的年度总费用;人口统计学特征;最昂贵和次要疾病;住院时间;发病率数量;每个 ICD10 章节(国际疾病分类,第 10 次修订版)的费用;以及昂贵治疗的使用(包括透析、移植手术、昂贵药物、重症监护病房和诊断相关组>€30000)。
前 1%和前 2%-5%的受益人分别占总支出的 23%和 26%。在前 1%的受益人中,医院护理占支出的 76%,其中昂贵药物和 ICU 护理分别占 9.0%和 9.1%。我们发现,54%的前 1%受益人年龄在 65 岁或以下,并且在前 1%组中,年龄越高,平均成本急剧下降。昂贵的治疗方法导致三分之一的前 1%受益人以及不到 10%的前 2%-5%受益人产生高额费用。前 1%和前 2%-5%受益人的平均疾病数量分别为 5.5 和 4.0。53%的前 1%受益人患有循环系统疾病,但对于只有 22%的前 1%受益人来说,这是他们最昂贵的疾病。
昂贵的治疗方法、最昂贵的疾病和年龄被证明是研究这一异质人群的有用变量。昂贵的治疗方法在前高费用受益人中发挥了重要作用。干预措施需要针对所有年龄段的受益人;仅仅关注老年人将使许多高费用受益人得不到解决。需要制定有针对性的干预措施来满足高费用受益人的需求,并避免浪费稀缺资源。