Bichoupan Kian, Tandon Neeta, Crismale James F, Hartman Joshua, Del Bello David, Patel Neal, Chekuri Sweta, Harty Alyson, Ng Michel, Sigel Keith M, Bansal Meena B, Grewal Priya, Chang Charissa Y, Leong Jennifer, Im Gene Y, Liu Lawrence U, Odin Joseph A, Bach Nancy, Friedman Scott L, Schiano Thomas D, Perumalswami Ponni V, Dieterich Douglas T, Branch Andrea D
Division of Liver Diseases, Icahn School of Medicine at Mount Sinai, New York, NY 10029, United States.
Janssen Scientific Affairs, LLC, Titusville, NJ 08560, United States.
World J Virol. 2017 Nov 12;6(4):59-72. doi: 10.5501/wjv.v6.i4.59.
To assess the real-world effectiveness and cost of simeprevir (SMV), and/or sofosbuvir (SOF)-based therapy for chronic hepatitis C virus (HCV) infection.
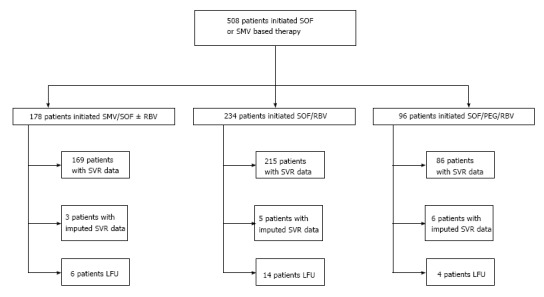
The real-world performance of patients treated with SMV/SOF ± ribavirin (RBV), SOF/RBV, and SOF/RBV with pegylated-interferon (PEG) were analyzed in a consecutive series of 508 patients with chronic HCV infection treated at a single academic medical center. Patients with genotypes 1 through 4 were included. Rates of sustained virological response - the absence of a detectable serum HCV RNA 12 wk after the end of treatment [sustained virological response (SVR) 12] - were calculated on an intention-to-treat basis. Costs were calculated from the payer's perspective using Medicare/Medicaid fees and Redbook Wholesale Acquisition Costs. Patient-related factors associated with SVR12 were identified using multivariable logistic regression.
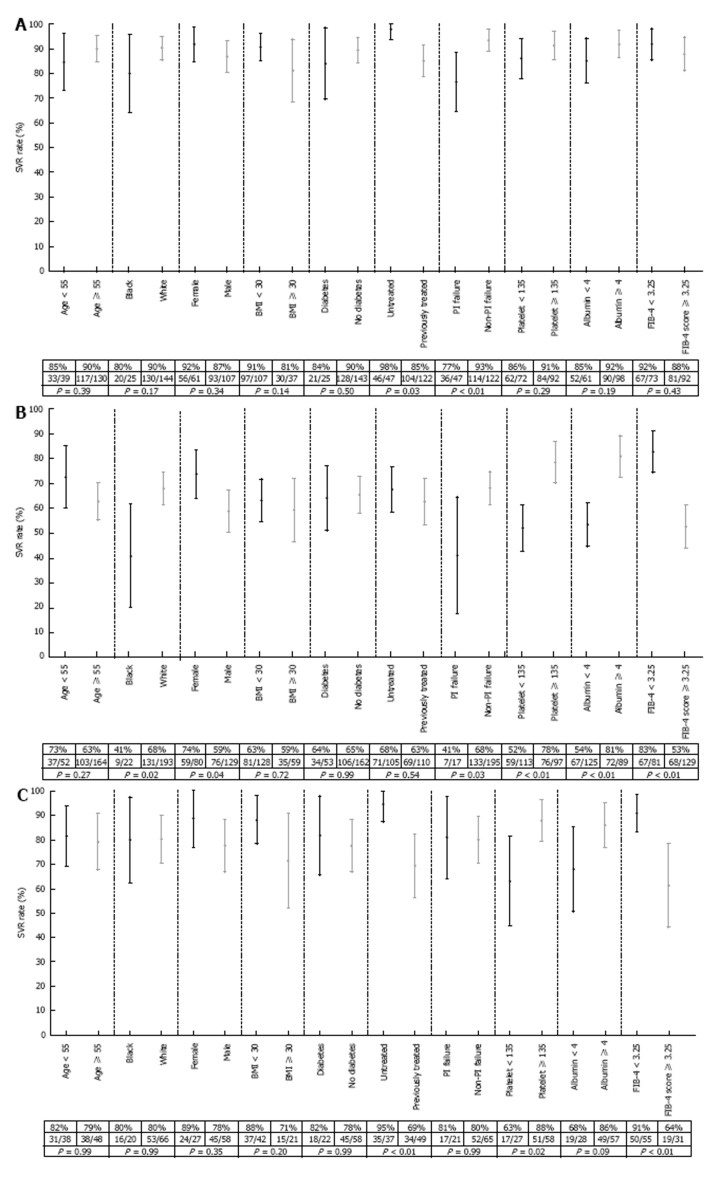
SVR12 rates were as follows: 86% (95%CI: 80%-91%) among 178 patients on SMV/SOF ± RBV; 62% (95%CI: 55%-68%) among 234 patients on SOF/RBV; and 78% (95%CI: 68%-86%) among 96 patients on SOF/PEG/RBV. Mean costs-per-SVR12 were $174442 (standard deviation: ± $18588) for SMV/SOF ± RBV; $223003 (± $77946) for SOF/RBV; and $126496 (± $31052) for SOF/PEG/RBV. Among patients on SMV/SOF ± RBV, SVR12 was less likely in patients previously treated with a protease inhibitor [odds ratio (OR): 0.20, 95%CI: 0.06-0.56]. Higher bilirubin (OR: 0.47, 95%CI: 0.30-0.69) reduced the likelihood of SVR12 among patients on SOF/RBV, while FIB-4 score ≥ 3.25 reduced the likelihood of SVR12 (OR: 0.18, 95%CI: 0.05-0.59) among those on SOF/PEG/RBV.
SVR12 rates for SMV and/or SOF-based regimens in a diverse real-world population are comparable to those in clinical trials. Treatment failure accounts for 27% of costs.
评估simeprevir(SMV)和/或sofosbuvir(SOF)为基础的疗法用于慢性丙型肝炎病毒(HCV)感染的实际疗效和成本。
在一家学术医疗中心连续治疗的508例慢性HCV感染患者中,分析接受SMV/SOF±利巴韦林(RBV)、SOF/RBV以及SOF/PEG/RBV治疗患者的实际治疗效果。纳入基因1至4型患者。在意向性治疗基础上计算持续病毒学应答率(治疗结束12周后血清HCV RNA检测不到,即持续病毒学应答12周[SVR12])。从支付方角度,使用医疗保险/医疗补助费用及《红皮书》批发采购成本计算成本。通过多变量逻辑回归确定与SVR12相关的患者因素。
SVR12率如下:178例接受SMV/SOF±RBV治疗的患者中为86%(95%CI:80%-91%);234例接受SOF/RBV治疗的患者中为62%(95%CI:55%-68%);96例接受SOF/PEG/RBV治疗的患者中为78%(95%CI:68%-86%)。每例SVR12的平均成本,SMV/SOF±RBV为174442美元(标准差:±18588美元);SOF/RBV为223003美元(±77946美元);SOF/PEG/RBV为126496美元(±31052美元)。在接受SMV/SOF±RBV治疗的患者中,既往接受过蛋白酶抑制剂治疗的患者获得SVR12的可能性较小[比值比(OR):0.20,95%CI:0.06-0.56]。较高胆红素水平(OR:0.47,95%CI:0.30-0.69)降低了接受SOF/RBV治疗患者获得SVR12的可能性,而FIB-4评分≥3.25降低了接受SOF/PEG/RBV治疗患者获得SVR12的可能性(OR:0.18,95%CI:0.05-0.59)。
在不同的实际临床人群中,以SMV和/或SOF为基础的治疗方案的SVR12率与临床试验中的相当。治疗失败占成本的27%。