Ling Andrew, Furhang Eli, Ryemon Shannon N, Ennis Ronald D
Department of Radiation Oncology, Mount Sinai West Hospital, New York, New York.
Icahn School of Medicine at Mount Sinai, New York, New York.
Adv Radiat Oncol. 2017 Sep 8;2(4):615-623. doi: 10.1016/j.adro.2017.09.005. eCollection 2017 Oct-Dec.
We retrospectively analyzed late small bowel toxicity in patients who received abdominal or pelvic intensity modulated radiation therapy (IMRT) to the small bowel with a maximum dose greater than the generally accepted maximal tolerable dose of 45 Gy.
All patients (N = 94) who received IMRT with a point dose of at least 45 Gy to tightly contoured small bowel between 2005 and 2014 at our institution were included. The median prescribed treatment dose was 70.2 Gy. The median follow-up was 20.1 months. Late small bowel toxicity was assessed using the Common Terminology Criteria for Adverse Events Version 3.0. Dosimetric variables and clinical factors were assessed for their relationship to small bowel toxicity.
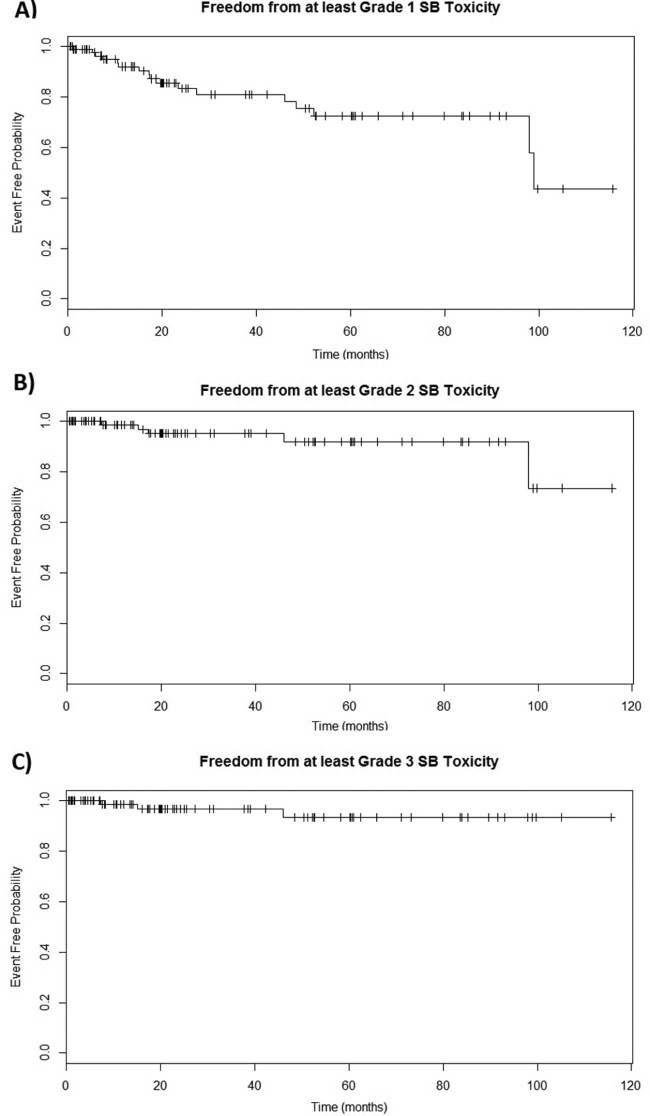
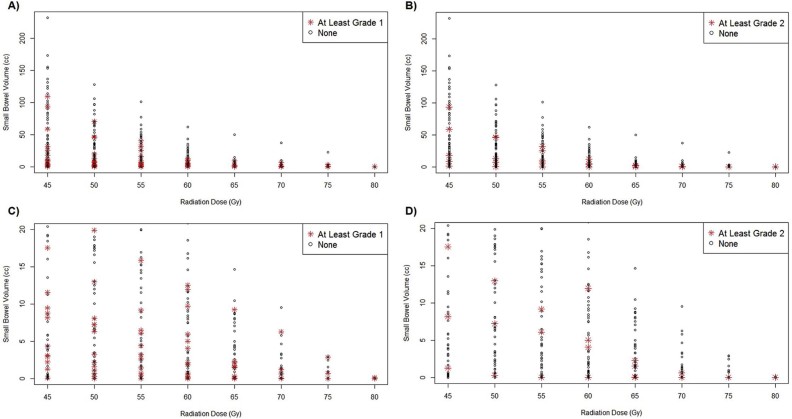
The median maximal small bowel point dose (D) was 6546.5 cGy. The estimated 5-year rates of freedom from at least grade 1, at least grade 2, and at least grade 3 late small bowel toxicity were 72.4% (95% confidence interval [CI], 60.7%-86.5%), 91.9% (95% CI, 84.1%-100%), and 93.6% (95% CI, 86.2%-100%), respectively. One patient (1.1%) developed grade 3 late toxicity, and 2 patients (2.1%) developed grade 4 late toxicity. Use of capecitabine/5-fluorouracil treatment was a significant predictor (<0.001) of at least grade 1 and at least grade 2 small bowel toxicity. No other clinical factors were associated with toxicity. None of the dose-volume parameters were significant predictors of small bowel toxicity.
It may be possible with IMRT to deliver high doses to small volumes of small bowel with low rates of significant long-term complications. Further studies should explore tolerable dose-volume relationships in cases in which aggressive abdominal or pelvic treatment may be warranted to treat the underlying malignancy.
我们回顾性分析了接受腹部或盆腔调强放射治疗(IMRT)的患者的晚期小肠毒性,这些患者小肠接受的最大剂量超过了普遍认可的45 Gy最大耐受剂量。
纳入了2005年至2014年在我们机构接受IMRT且小肠紧密轮廓处点剂量至少为45 Gy的所有患者(N = 94)。规定治疗剂量的中位数为70.2 Gy。中位随访时间为20.1个月。使用不良事件通用术语标准第3.0版评估晚期小肠毒性。评估剂量学变量和临床因素与小肠毒性的关系。
小肠最大点剂量(D)的中位数为6546.5 cGy。至少1级、至少2级和至少3级晚期小肠毒性的估计5年无病生存率分别为72.4%(95%置信区间[CI],60.7%-86.5%)、91.9%(95%CI,84.1%-100%)和93.6%(95%CI,86.2%-100%)。1例患者(1.1%)发生3级晚期毒性,2例患者(2.1%)发生4级晚期毒性。使用卡培他滨/5-氟尿嘧啶治疗是至少1级和至少2级小肠毒性的显著预测因素(<0.001)。没有其他临床因素与毒性相关。没有一个剂量体积参数是小肠毒性的显著预测因素。
通过IMRT有可能向小体积小肠输送高剂量,且严重长期并发症发生率较低。进一步的研究应探索在可能需要积极的腹部或盆腔治疗以治疗潜在恶性肿瘤的情况下可耐受的剂量体积关系。