Jaafar Gona, Darkahi Bahman, Lindhagen Lars, Persson Gunnar, Sandblom Gabriel
Department of Clinical Sciences, Intervention and Technology (CLINTEC), Karolinska Institutet, Center for Digestive Diseases, Karolinska University Hospital, -141 86, Stockholm, SE, Sweden.
Department of Surgery, Enköping Hospital, Kungsgatan 71, 74538, Enköping, Sweden.
BMC Surg. 2017 Dec 6;17(1):128. doi: 10.1186/s12893-017-0312-0.
Antimicrobial resistance may be promoted by divergent routines and lack of conformity in antibiotic treatment, especially regarding the practice of antibiotic prophylaxis. The aim of the present study was to assess differences in gallstone surgery regarding antibiotic use in Sweden.
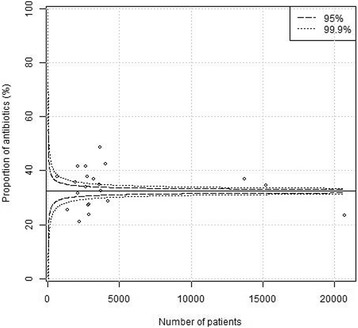
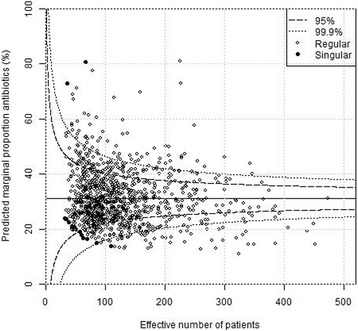
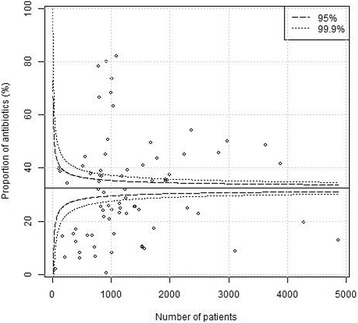
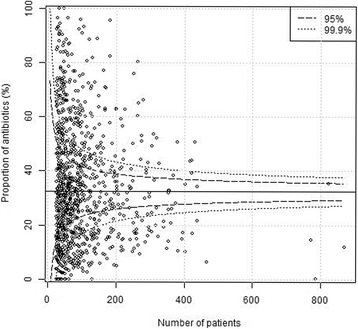
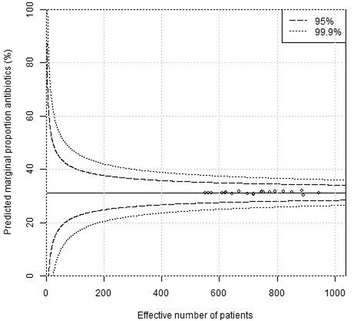
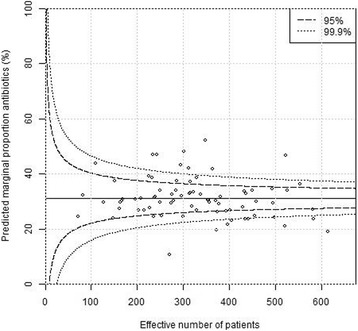
The study was based on data from the Swedish Register for Gallstone Surgery and ERCP (GallRiks) 2005-2015. Funnel plots were used to test impact of grouping factors, including, hospital and surgeon and to identify units that deviated from the rest of the population.
After adjusting for cofounders including age, gender, ASA classification, indication for surgery, operation time, gallbladder perforation and emergency status, there were 0/21 (0%) at the regional level, 18/76 (24%) at the hospital level and 128/1038 (12%) at the surgeon level outside the 99.9% confidence interval (CI). The estimated median odds ratios were 1.13 (95% CI 1.00-1.31) at the regional level, 1.93 (95% CI 1.70-2.19) at the hospital level and 2.38 (95% CI 2.26-2.50) at the surgeon level.
There are significant differences between hospitals and surgeons, but little or no differences between regions. These deviations confirm the lack of standardization in regards to prescription of antibiotic prophylaxis and the need more uniform routines regarding antibiotic usage. Randomized controlled trials and large population-based studies are necessary to assess assessing the effectiveness and safety of antibiotic prophylaxis in gallstone surgery.
抗生素治疗中不同的常规做法和缺乏一致性可能会促进抗菌药物耐药性的产生,尤其是在抗生素预防的实践方面。本研究的目的是评估瑞典胆结石手术中抗生素使用的差异。
该研究基于瑞典胆结石手术和内镜逆行胰胆管造影登记处(GallRiks)2005 - 2015年的数据。漏斗图用于测试分组因素的影响,包括医院和外科医生,并识别与其他人群存在偏差的单位。
在对包括年龄、性别、美国麻醉医师协会(ASA)分级、手术指征、手术时间、胆囊穿孔和急诊状态等混杂因素进行调整后,区域层面超出99.9%置信区间(CI)的有0/21(0%),医院层面有18/76(24%),外科医生层面有128/1038(12%)。区域层面估计的中位数优势比为1.13(95%CI 1.00 - 1.31),医院层面为1.93(95%CI 1.70 - 2.19),外科医生层面为2.38(95%CI 2.26 - 2.50)。
医院和外科医生之间存在显著差异,但区域之间差异很小或没有差异。这些偏差证实了抗生素预防处方缺乏标准化,以及需要更统一的抗生素使用常规做法。需要进行随机对照试验和基于大人群的研究来评估胆结石手术中抗生素预防的有效性和安全性。